Author Contributions
Academic Editor: Alyaa Ragaei, Ass. Prof. of general Histology, supplementary general science, Faculty of Oral and Dental Medicine, Future University in Egypt (FUE).
Checked for plagiarism: Yes
Review by: Single-blind
Copyright © 2018 Abbas Alnaji
 This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Competing interests
The authors have declared that no competing interests exist.
Citation:
Introduction
It is an honor to write in a big mankind health problem hence I am Neurosurgeon. It is routine to send my neurosurgical patients whom suffer from Diabetes Mellitus DM to a related specialties to help in regulating or overcome high blood sugar which form a real recovery obstacle especially with my attitude where I deal with or consider all neurosurgical problems as a medico-surgical issues of a long standing Intra-cellular bacterial ICB nature. A certain percentage remain with uncontrolled DM Inspite of expert management. Whence I found many solutions for neurological and neurosurgical problems away from symptomatic and palliative managements based on a deep clinical and then laboratory basis these problems being mere complications to a long standing silent, dormant or sub-clinical ICB infections on which a trial treatments gave an excellent results without non-steroidal analgesics, steroids, sedatives including antidepressants and many others. A phenomenon arose in these patients with uncontrolled DM (like having 60 IU of insulin per day and their random blood sugar is around 450 mg/ 100 ml) by experience of dizziness, sweating and other symptoms and signs of hypoglycemia in a variable time interval less than month from the start of the anti-bacterial for a given case of my field, I instruct them to lower insulin intake they recur to this “problem” according to their mind or thinking, after it being faded! I ask for more lowering of insulin until no insulin is needed any more in several patients of such kind where as the mild to moderate cases of DM are much more or let me say ‘many whom treated with this concept and become insulin free’. Here the quantity is not the governor in face of the nature or quality where wisdom states “EVERY POT LEAKS OR DROPS WHAT WITH IN” https://en.wikipedia.org/wiki/Ali which means even a single case if so is enough to guide us to the beginning of the string just we have to follow. As I am not a DM specialist I asked a physician (GP) colleague to apply after I discussed him the matter the result in one case of such severe type was similar to mine the astonishing in the matter he regret to continue and become silent when I ask him why not to proceed further!!! Another strange situation the head (in certain period) of our teaching hospital BM and endocrine center who is consultant in medicine refused to cooperate just when he heard that I have what make DM management more realistic Inspite of he knows my scientific capabilities and research attitude. As I am selfish I preferred to publish this issue then start to ask for local and foreign real cooperation especially when I start to write in the remote effects of ICB invasion into our cells where this concide with. So the matter is cellular events rather than Biochemical or an error in the metabolism of carbohydrate and type I and II or others. Insulin in its journey from Beta cells production to the target cells receptors defect is a level. The other level is ’’ what behind the target cells receptor’’. It is known for some extent her or there that infection affect BM reciprocally. This concept denotes the extracellular infections mostly. I stress on or deal with Intra-cellular infection and of Bacterial type where viruses and fungus are put a side due to our capacity is so limited to widen the front or add more variables to the equation I may talk or consider after a real support from the mankind efforts to dip deep in these regards. Insulin production may be defective in quantity or quality after Pancreatic affection as a complication to the long standing ICB infection. Those whom got better or their uncontrolled DM become controlled or some become insulin free that’s to say not Diabetic any more they treated by me for some other Neurological or Neurosurgical entities with anti-Brucella trial treatment on clinical bases and then some showed positive PCR open Sacro-iliac joint tissue or Trapezius muscle biopsies. So why THIS, is not part of, THAT!! The improvement by simple logic is due to the suitable anti-Brucella where overcome the infection that caused the so many symptomatology as remote complications and so the DM is another or additional complication set. The negative to this logic seems that the condition is or became irreversible because of the long standing affection by ICB not due unknown or what else! So if the insulin produced is defective in its molecular structure that do not fit the target receptor properly or the general infectious state (sick cell syndrome that result from the other cells affection) that make these other cells produce chemicals hostile to the insulin in their transit all make BM in different grades.
By coming to the target cells receptor wise, here we may find extra-cellular issue, and what I called “what behind the target cells receptor’’ level or issue. The extra-cellular deformity in the receptor molecular configuration I think cannot be separated from that of the is “what behind the target cells receptor’’ but we may find a hostile chemicals that block or make blockade that make insulin antagonists or even some structural deformities these chemicals like that of insulin molecule neutrants (from neutralization) produced from altered functionality of our cells that harbor the long standing ICB as a type of the negative adaptation to the invader.
“what behind the target cells receptor’’ let us discuss this by mentioning the following very popular scheme. The door bell of any type as what in the ancient ages a rope with a some sort of a handle outside and a metallic classical bell inside where it is heard by the household or recently the electric bell a button out and the magnet forming electric coil inside the house. It is not simple just by the rope or wire crossing the house wall (receptor molecule crosses the cell wall) where the bulk is inside. This bulk is the system inside the cell connected with the receptor from within that bring to a cascade of events enabling the glucose molecule to enter this cell for fueling it. I do not know what it is exactly and guessing no one can too! Rather, I want to discuss philosophically what could happen in these Microsystems as faults or defects from our point of view making our cells whom are target for insulin-glucose manner deviate toward some side left or right which we know any deviation to any side called a disease in medicine. This deviation could be a planned from or a need from the invasive ICB point of view, and I do not need to mention we are so poor in understanding what is the limit (aim to which ICB works to) so no need to hear, ICB deprive its self from fuel by this!! Glucose could not be fuel to ICB and by stop its entry to the our cells making the later in a weakness due to this sort of blockade!! The intra-cellular system triggered by sound insulin-receptor coupling is of a given physiology as I mentioned earlier whether we know it in full or in less is changed by the long standing presence of ICB certainly toward the benefit of ICB, this is by logic. To come to lab proves I started to cooperate with an electron-microscope specialist just to see, what could be seen by this machine and try to explain. The aim is to see what is went on when the patient was in uncontrolled DM and then when become controlled or insulin need free as I mentioned earlier when anti-Brucella was given in the beginning of my career in this regard, and then I admitted tissue screen for possible other intra-cellular bacterial infection as it become clearer when I put a list for possible other ICB which are checked with Micro-array molecular system I found two bacteria in a single Trapezius biopsy after 45 days in this patient who was treated for Brucella on clinical ground very successfully that is to say it could be three were cooperating or not to produce her long standing clinical manifestations which become annoying before I consulted for and in non-neurosurgical issue Inspite of many specialized prescriptions. Indeed I ask for cooperation from anywhere.

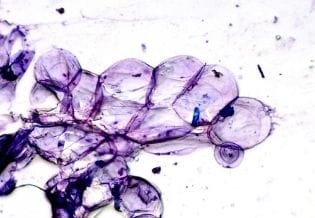
Micro-array test on Trapezius muscle open biopsy in a 50 years old female suffering from annoying scalp suppurative boils and dermatitis many regimens of dermatological therapies failed for six months with progressive deterioration. Seven days patient become with excellent improvement on anti-Brucella on clinical basis ( I know the long history of this patient as she is relative suffering from different vague psycho-somatic manifestations so long before to end with this, her general health is very poor as if she is looking in eighties of age with severe weight loss but not Diabetic and not with neoplasm as she was worked up). PCR test on same sample is negative done with micro-array 45 days after the beginning of the treatment.