
Abstract
Objectives
To evaluate the diagnostic accuracy of chest CT for the diagnosis of COVID-19 associated with the clinical presentation and in relation to the PCR-RT. Sensitivity, specificity, positive predictive value and negative predictive value, gender, age group and degree of lung involvement will be evaluated.
Methods
We evaluated 1545 patients with chest CT, delineating the age range and degree of lung involvement, and 306 patients with chest CT and PCR-RT.
Results
Of the 1545 examinations, 53% were men and 47% were women, there was greater involvement in the 50-59 age group. In the pulmonary study, 55.05% were COVID-19. In the degree of lung involvement 37.70% were mild, 35.76% were moderate, and 26.54% were severe. In the distribution by age, there was a greater involvement between 50-59 years with 56% between moderate (27.6%) and severe (28.0%). Between tomography and PCR-RT, the sensitivity was 68.8%, specificity 59.5%, accuracy 91.3%, with prevalence 31.9%, positive predictive value 44.3% and negative predictive value 80.3%, in females, sensitivity 55.3%, positive predictive value 37.1%, negative predictive value 75.3%, in males, sensitivity 81.6%, positive predictive value 50, 6 and negative predictive value 86.6%.The sensitivities are different between the genders with p of 0.005 and specificity of 0.938, with age effect, starting at 45 years we have a p of 0.057 that decreases to 0.006 at 80 years for sensitivity and specificity.
Conclusions
The sensitivity and accuracy of CT scan in relation to PCR-RT was significant. Sensitivity increases with prevalence and in the older age group and in men.
Author Contributions
Academic Editor: Ian James Martins, Edith Cowan University, USA
Checked for plagiarism: Yes
Review by: Single-blind
Copyright © 2022 Gleim Dias de Souza, et al.
 This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Competing interests
The authors have declared that no competing interests exist.
Citation:
Introduction
The 2019 outbreak of pandemic coronavirus disease (COVID-19) has opened a window into an unexpected world. The prevalence of COVID-19 has gone from 0% to an unknown but certainly high proportion of the population. This prevalence is also changing over time in different parts of the world 1
The presence of irregular and/or confluent band-like ground-glass opacity or consolidation in a peripheral and middle to lower lung zone distribution on a chest CT scan obtained in the setting of pandemic COVID-19 is highly suggestive of SARS-CoV-2 infection and should be used in conjunction with clinical judgment to make a diagnosis 2
Because of the primary involvement of the respiratory system, chest CT is strongly recommended in suspected cases of COVID-19, both for initial and follow-up evaluation. Chest radiographs are of little diagnostic value in the early stages, whereas CT findings may be present even before the onset of symptoms. In the intermediate to advanced stages of the disease, chest radiographs can show the progression of acute respiratory distress syndrome (ARDS) features, in addition, CT findings have proven diagnostic in several cases with an initial screening test with reverse transcription polymerase chain reaction (RT-PCR) 3. Computational intelligence approaches further strengthen the power of imaging tools and help medical experts in the global fight against COVID-19 with the help of clinical imaging, such as X-rays and CT scans1.
The gold standard for COVID-19 diagnostic screening is PCR-RT(3,45), PCR-RT test is a commonly used and highly specific messenger RNA detection and quantification technique that can detect the presence of SARS-COV-2 in a sample 4 Noteworthy is the paucity in the number of tests available and the increased time between the collection of the test and its effective result in this time, medical imaging such as computed tomography offers great potential as an alternative 7 In the current pandemic context and the practical difficulty in using RT-PCR, the high prevalence of clinical symptoms was taken into consideration for the indication of tests and examinations that confirm the diagnostic hypothesis quickly and reliably. Patients with a clinical picture suggestive of COVID-19 associated with chest CT findings compatible with SARS-CoV-2 infection have been shown to have a high positive predictive value as well as high accuracy for the diagnosis of COVID-19 5, 6, 7. The association of highly suggestive symptoms for COVID-19 with specific tomographic findings can be shown to have specificity of up to 96.6%8, a value very similar to RT-PCR tests used worldwide 2, 3, 4, 6.
Thus chest CT scanning has been used in symptomatic patients assisting for effective diagnosis, classification, evaluation of improvement and worsening, as well as sequelae, and this has been a focus of debate and studies worldwide.
Objectives
To evaluate the diagnostic accuracy of chest CT for the diagnosis of COVID-19 associated with clinical picture in relation to PCR-RT.
Sensitivity, specificity, positive predictive value and negative predictive value, gender, age group and degree of lung involvement will be evaluated.
Methods
The present study was approved by the Research Ethics Committee of the Fundação de Ensino e Pesquisa FEPECS/Escola Superior de Ciências da Saúde ESCS and Universidade Federal de São Paulo/UNIFESP. All participants were exempted from signing the informed consent form.
The patients came from the emergency care of the HRAN Hospital, reference for the care of COVID-19 in the city of Brasilia - Federal District, in the period from March 15 to June 15, 2020, phases of the pandemic beginning until its peak period of care, by spontaneous search, when presenting symptoms suggestive of COVID-19 as anosmia, fever, myalgia, sore throat and others. Routinely requested tests for diagnostic clarification were used in the research.
A prospective analytical study of 1545 symptomatic clinical patients in diagnostic research for COVID-19 was performed, with suggestive clinical presentation, characterizing inclusion criteria, and PCR-RT and high-resolution chest CT were requested.
The exclusion criteria of the protocol were patients without evident symptoms suggestive of COVID-19.
Tomographic Evaluation
All 1545 patients underwent High Resolution Computed Tomography of the Chest. The HRCT were performed in Toshiba Aquilion® XLT 128 channel and Canon® 16 channel scanners. All images were obtained at maximum inspiration, using 0.5 to 1.5 mm collimation, with 120 kV and automatic mAs dose modulation. The intervals between images were 5 to 10 mm, with the patient in supine and prone position. Evaluation by two expert radiologists with more than 20 years of experience in the analysis of CT scans with a specialist title was characterized in grouping the patients as follows:
1-NORMAL group: Patients evaluated without evident pulmonary changes by the method.
2-Other group: Patients evaluated with pulmonary changes characteristic of other pathologies.
3-Group COVID-19: Patients evaluated with pulmonary changes characteristic of COVID-19.
In this group, besides the qualitative evaluation, a quantitative analysis was performed, subdividing the lungs into three parts, characterized as mild involvement (up to 25% of the lung area), moderate (from 25 to 50% of the lung area) and severe (between 50 and 100% of the lung area).
Evaluation by PCR-RT
PCR-RT testing at the time of the pandemic was not available for all patients, and 306 patients had PCR-RT testing performed in conjunction with CT scanning.
Etiologic detection, including nucleic acid detection and antigen detection, can be used as a means to confirm the presence of pathogens, but the detection rate is affected by several factors, such as sampling, storage, and reagent performance. Especially in the application of COVID-19 detection, widely used throat swabs are affected by many factors that limit detection rates, including the immune status of the body's immune system, the specificity of the pathogen's target organs, and disease progression 1.
The (KIT MOLECULAR SARS-CoV2 (E) - Bio-Manguinhos was used by swab collection of samples of respiratory secretions from the nose and throat. The swab is a type of plastic rod with cotton swabs on the tips. The SARS-CoV2 Molecular Kit - Bio-Manguinhos is based on Real-Time PCR technology and is indicated for the processing of clinical samples, previously submitted to the nucleic acid extraction step.
Analytical sensitivity in PROBIT analysis (95% CI) indicated a sensitivity for target E: LOD of 0.97 copies/reaction (50% positivity) and of 1.99 copies/reaction (95% positivity). Summarizing, the limit of detection for Coronavirus was established: 50 copies/reaction.
Evaluation By High Resolution Computed Tomography of The Chest
1545 symptomatic individuals underwent computed tomography. Therefore, we will perform a demographic analysis of the data obtained from these patients, characterizing sex, age group and degree of pulmonary involvement.
Joint Evaluation Between Computed Tomography and PCR-RT
Of the 1545 symptomatic individuals analyzed, 306 individuals underwent high resolution chest computed tomography and PCR-RT, and statistical analysis was performed referencing the two methods.
Statistical Analysis
To describe the quantitative variables, the statistics of mean, median, minimum value, maximum value, and standard deviation were considered. To summarize the qualitative variables, frequencies and percentages were considered. The measures of sensitivity, specificity, accuracy, positive predictive value, and negative predictive value were those considered in assessing the quality of CT scans for the diagnosis of Covid-19.
For comparison of two classes of a variable in relation to a quantitative variable, Student's t test for independent samples was considered. For evaluation of the association of two qualitative variables, the chi-square test was considered.
To evaluate the joint association of gender and age on sensitivity and specificity measures, the Logistic Regression model was adjusted. P values lower than 0.05 indicated statistical significance.
Results
Analysis of The Patients Who Underwent Chest High Resolution Computed Tomography
In the analysis of 1545 individuals who underwent high-resolution chest CT, 53% were men and 47% were women, with respect to the age range, it was significant in all age groups, with a predominance in the age groups between 30-39 and 60-69 years, being higher in the range of 50-59 years.
In the analysis of lung involvement, 32.45% were considered normal, 12.50% showed changes characteristic of other diseases and 55.05% showed changes characteristic of COVID-19. Regarding the degree of involvement, 37.70% had their pulmonary changes characterized as mild involvement (up to 25% of the lung area), 35.76% moderate (impairment of 25 to 50% of the lung area) and 26.54% severe (between 50 and 100% impairment of the lung area).
The age distribution of patients affected by covid-19 was predominantly from 30-39 to 50-59 years, with greater involvement between 50-59 years with 56% of patients classified between moderate (27.6%) and severe (28.0%).
Analysis of Patients Who Underwent High-Resolution Chest Computed Tomography and PCR-RT
Tomography Quality Measures in the Diagnosis of Covid-19 Considering Pcr Result As Gold Standard
In the analysis of high-resolution chest CT scan in the diagnosis of covid-19, considering the RT-PCR result as the gold standard, 301 individuals were studied (Figure 1: A1 and B1) showing CT scan sensitivity of 68.8%, with specificity of 59.3%, accuracy of 91.3%, with a prevalence of 31.9% and having a positive predictive value of 44.3% and a negative predictive value of 80.3%. In the graph can be seen the positive predictive value and negative predictive value for different prevalence values.
Figure 1.(A1): prevalence of COVID-19 to positive predictive values in CT (CT with PCR-RT as gold standard. (B1): VP+ and VP- estimates of COVID-19 on CT with PCR-RT as gold standard.
Evaluation of The Effect of Sex on Covid-19 Diagnosis By Tomography Considering PCR As The Gold Standard
Tomography Quality Measures - Female Gender
In the evaluation of the effect of female sex on the diagnosis of covid-19 by high-resolution chest CT scan considering the RT-PCR result as the gold standard, (Figure 2: A2 and B2) 155 individuals were studied showing a sensitivity of 55.5%, with specificity of 59.3%, accuracy of 82.6%, with a prevalence of 30.3 % and having a positive predictive value of 37.1% and a negative predictive value of 75.3%.
Figure 2.(A2): VP+ and VP- for different prevalence values on CT with PCR-RT in females. (B2); Estimates of different prevalence in CT with PCR-RT as gold standard in females.
Tomography Quality Measures - Male Gender
In evaluating the effect of male sex on high-resolution chest CT scanning in the diagnosis of covid-19, considering the RT-PCR result as the gold standard (Figure 3: A3 and B3), 146 individuals were studied showing a sensitivity of 81.6%, with specificity of 59.8%, accuracy of 100%, with a prevalence of 33.6 % and having a positive predictive value of 50.6% and a negative predictive value of 86.6%.
Figure 3.(A3): VP+ and VP- for different prevalence values on CT evaluation with PCR-RT in males. (B3); Estimates of different prevalence in CT evaluation with PCR-RT as gold standard in males.
Evaluation of The Effect of Gender on Tomography Quality Measures in The Diagnosis of Covid-19
Sensitivity
We tested the null hypothesis of equal sensitivity in both sexes versus the alternative hypothesis of different sensitivities, with p value of 0.005 characterizing that there is a difference in sensitivity between the genders.
Specificity
The null hypothesis of equal specificity in both sexes versus the alternative hypothesis of different specificities was tested, with p value of 0.938 characterizing that there is no significant difference between the genders. Figure 4
Figure 4.(A4 and B4) shows the sensitivities estimated by the model and observed, for different age groups within each sex.
Evaluation of The Effect of Gender On Tomography Quality Measures in The Diagnosis of Covid-19 Controlling For Patient Age
Sensitivity
We initially tested the null hypothesis that the effect of age on sensitivity is equal in both sexes versus the alternative hypothesis that the effect of age on sensitivity is different in both sexes. The result of the statistical test indicated non-rejection of the null hypothesis (p=0.065).
Due to the tendency to reject the null hypothesis of different effects of age on sensitivity in the two groups and also due to the good fit of the model with different effects (p=0.897) this model was considered in the subsequent analysis.
With these results, of different effects of age on sensitivity in the two sexes, for each particular age (Figure 5: A5 and B5) we tested the null hypothesis of equal sensitivities in the two sexes versus the alternative hypothesis of different sensitivities. The table below shows the estimates of sensitivities for each age group according to sex, as well as the p-value of the statistical test.
Figure 5.(A5) Sensitivity estimates for each age group according to sex, as well as the corresponding p value. (B5). Male (continuous) and female (dasched), sensitivity curves in relation to age group according to sex, as well as the corresponding p value.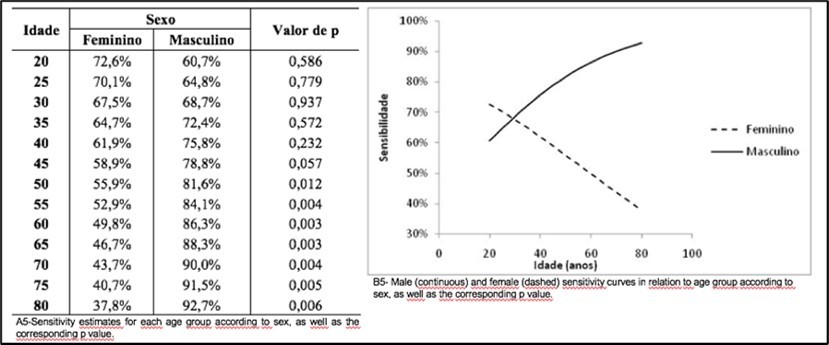
Specificity
Initially, the null hypothesis that the effect of age on specificity is equal in both sexes versus the alternative hypothesis that the effect of age on specificity is different in both sexes was tested. The result of the statistical test indicated failure to reject the null hypothesis (p=0.693).
Given this result, the null hypothesis of no association of age with specificity was tested versus the alternative hypothesis of the existence of an association. The result of the statistical test indicated the non-rejection of the null hypothesis (p=0.479).
In table 6 and graphic 6 right below it can be seen the specificities estimated by the model and observed, for different age groups inside each sex. (Figure 6)
In the presence of patient age, the null hypothesis of equal specificity in both sexes versus the alternative hypothesis of different specificities was tested. The result of the test indicated non-rejection of the null hypothesis (p=0.930).
Figure 6.(A6) - Specificities for different age groups in males and females. (B6) - Specifics for different age groups in males and females
Evaluation of The Relationship Between Patient Age and Ct Scan Results
Sensitivity
In cases with positive CRP we tested the null hypothesis of equal mean age in cases with negative CT scan result and in cases with positive CT scan result versus the null hypothesis of different means with p of 0.720 characterizing that there is difference in mean age between positive and negative CT scan cases.
Specificity
In cases with negative CRP we tested the null hypothesis of equal mean age in cases with negative CT scan results and in cases with positive CT scan results versus the null hypothesis of different means, with p of 0.458 characterizing that there is a difference in mean age in cases with negative CT scan results and in cases with positive CT scan results.
Comparison of The Genders in Relation to the Age of The Patient
We tested the null hypothesis of equal mean age in male cases and female cases versus the null hypothesis of different means with p 0.408 characterizing the difference between the sexes in relation to the patient's age in the evaluations performed.
Prevalence of Covid Considering The Age And Sex of The Patient Considering The Positivity in The Result Of PCR
The prevalence of COVID-19 was evaluated in relation to the female gender and age group considering the positivity in the PCR/CT scan result, observing a prevalence of 31.6% up to 30 years of age, in the 31 to 50 years range the prevalence was 35.6%, in the 51 to 70 years range it was 25.0% and over 70 years it was 28.0%. (table 7, chart 8)
In males, up to 30 years old was 26.7%, from 31 to 50 years old was 35.1%, from 51 to 70 years old was 32.1%, and above 70 years old was 40.0%. (Figure 7: (A7 and B7)
Figure 7.(A7) Prevalence of COVID-19 considering the age and sex of positive patients in the PCR-RT. (B7): Prevalence of COVID-19 considering the age and sex of patients.
Discussion
Images of multiple, unequal areas of ground-glass opacity and consolidation predominantly in the periphery of the lungs are characteristic manifestations at chest CT and are extremely useful in the early detection and diagnosis of this disease, aiding in the immediate diagnosis and eventual control of this global health emergency2. The lesions are mainly distributed in the lower lobes and in the peripheral zone, and most of the peripheral lesions are accompanied by localized pleural thickening adjacent to the subpleural region 9, 10, 11, 12, 13, 14.
Several entities may present with similar imaging patterns, predominantly ground-glass opaque, and within specific contexts, one should include in the differential diagnosis other infections by atypical agents including opportunistic agents (other viral agents, Mycoplasma pneumoniae, Pneumocystis jirovecii and others), inflammatory interstitial involvement of the lung parenchyma (organizing pneumonia, diffuse alveolar damage) determined by collagenosis, drugs or others15,16. However patients with fever and/or cough and conspicuous ground-glass opacity lesions in the peripheral and posterior lungs on CT images, combined with normal or decreased WBCs and a history of epidemic exposure, are highly suspected of having 2019 New Coronavirus (2019 -nCoV) pneumonia17 . Chest CT has high sensitivity for the diagnosis of 2019 coronavirus disease (COVID-19). Chest CT can be considered the main tool for current detection of COVID-19 in epidemic areas 18.
Routine CT for the identification of COVID-19 pneumonia is not currently recommended by most radiology societies19. According to the CBR, the diagnosis of COVID-19 should be based on clinico-epidemiological information associated with RT-PCR and/or serology20. However, the number of chest CT scans performed on people under investigation for COVID-19 has increased. We also anticipate that some patients will have incidentally detected findings that can be attributed to COVID-19 pneumonia, requiring radiologists to decide whether or not to mention COVID-19 specifically as a differential diagnostic possibility19.
Patients with fever and/or cough and conspicuous ground-glass opacity lesions in the peripheral and posterior lungs on CT images, combined with normal or decreased WBCs and a history of epidemic exposure, are highly suspected of having 2019 New Coronavirus (2019 -nCoV) pneumonia21. COVID-19 chest CT detection is very high among symptomatic high-risk individuals, especially with thin-section chest CT. The most common CT features in patients affected by COVID-19 included ground-glass opacities and consolidation involving the bilateral lungs in a peripheral distribution22.
Sensitivity and specificity may vary in different clinical populations, and prevalence is a marker of these differences. Clinicians are advised to base their decisions on studies that most closely match their own clinical situation, using prevalence to guide the detection of differences in study population or study design23.
Diagnostic accuracy plays a central role in the evaluation of medical diagnostic tests. Test accuracy can be expressed as sensitivity and specificity, as positive and negative predictive values, or as positive and negative likelihood ratios. Some feel that the positive and negative predictive values of a test are more clinically relevant measures than sensitivity and specificity. However, predictive values depend directly on the prevalence of the disease and therefore cannot be directly translated from one situation to another. In contrast, it is believed that the sensitivity and specificity of a test do not vary with disease prevalence 24.
Several studies suggest that CT should be a primary diagnostic tool for coronavirus disease (COVID-19), as they have reported sensitivities with CT that are much higher than that of the reverse transcriptase polymerase chain reaction (RT-PCR) test25. The development of faster laboratory tests may limit the role of CT in the diagnostic evaluation of COVID-19. However, baseline CT has other applications and that demonstrate that the extent of lung abnormalities by CT on admission were predictors of recovery in the intensive care unit26. A negative CT should not be used to exclude the possibility of COVID-19, especially early in the disease. Later in the course of the disease, the frequency of consolidation increases27.
In our study, all patients with clinical symptoms were between the 2nd and 6th days from the onset of symptoms, and, for this reason, HRCT was performed together with high-resolution chest CT scan.
The comparison between HRCT and HR-CRP showed a sensitivity of 68.8%, with specificity of 59.5%, accuracy of 91.5%, positive predictive value of 44.3% and negative predictive value of 80.0%, with a prevalence in the study of 31.9%. The significantly higher prevalence compared to that of the Federal District (12.9%)28at that time is due to the fact that the hospital unit is a reference and receives patients from all over the Federal District and surrounding areas.
Regarding risk factors for the worsening of a disease, a review showed that the most severe cases of the disease that evolved to pneumonia were older patients, male and with comorbidities, when compared to milder cases29. Being male was a factor associated with a higher risk of dying from COVID-19. Men had a lower probability of survival than women, as well as a 45% higher risk of death than women. A systematic review with meta-analysis including nine studies described that men represent 60% of patients with COVID-19, indicating a higher susceptibility for virus infection in this population30.
COVID-19 shows a difference in the case fatality rate between men (2.8%) and women (1.7%) 31. When analyzing the female sex we obtained a sensitivity of 55.5%, specificity of 59.3%, accuracy of 82.6%, positive predictive value of 37.1 and negative predictive value of 75.3% with a prevalence in the study of 30.3%. In the male gender analysis, we obtained a sensitivity of 81.6%, specificity of 59.8, accuracy of 100.0%, positive predictive value of 50.6% and negative predictive value of 86.8% with a prevalence of 33.6%. When we evaluate the effect of the sex with the age group, we observed in the female sex a stability of the sensibility in the diverse age groups with a drop above 70 years old and in the case of the male sex a sensibility that increases, reaching 100.0%, above 70 years old in the male sex.
The global case fatality rate for confirmed cases of COVID-19 is approximately 6.9%. Although it is difficult to compare lethality rates between countries due to the different stages of the outbreak, and other variations such as age of patients, health status of the population, and the healthcare systems within each country 34. The southern United States experienced regional outbreaks of COVID-19 in June. In these regions, increases in the percentage of positive SARS-CoV-2 test results among adults aged 20-39 years preceded increases among adults ≥60 years by a mean of 8.7 days (range = 4-15 days), suggesting that younger adults likely contributed to community transmission of COVID-1932 In the study, the specificity analysis always remained above 50% in both sexes reaching 70% in patients over 70 years and under 30 years.
In the municipality of VO (Italy), the prevalence of infection ranged from a central estimate of 1.2% to 1.7% up to age 50 years. Older participants showed a threefold increase in the prevalence of infection. Of the 81 participants positive for SARS-CoV-2 in the two surveys, 13 required hospitalization (16.0%). The age distribution was as follows: 1 (7.7%) aged 41-50 years, 1 (7.7%) aged 51-60 years, 4 (30.8%) aged 61-70 years, 5 (38.5%) aged 71-80 years, and 2 (15.4%) aged 81-90 years 33.
Disease severity and outcome appear to be highly correlated with age of onset, where the most severe forms of COVID-19 were seen for adults ≥ 55 years 34, 35, 36, 37. Furthermore, an age-dependent mortality rate has been demonstrated with the lowest risk observed among those aged under 19 (0-0.1%) and 20-54 years (0.1-0.8%); however, the mortality risk gradually increases, affecting 1.4-4.9% in the 55-74 years age range, 4.3-10.5% among those aged 75-84 years, with the highest lethality rate of 10.4-27.3% in those aged ≥85 years (34,36,37,38). Individuals with underlying health problems such as cardiovascular disorders, diabetes, liver and kidney disease, malignant tumors, or suppressed immune system seem to contract the severe form of the disease and the increased mortality rate34, 35, 37. It is interesting that in the study, as of 45 years of age, we observed a decreasing p value, more significant up to 80 years of age, demonstrating the relevance of CT scanning as early as 45 years of age as an important tool in the diagnosis of COVID-19. In male individuals this sensitivity is higher and will certainly add to the clinical management to be taken. In the study we observed that the age averages vary in sensitivity and specificity, characterizing the importance of using high-resolution chest computed tomography in patients as a whole, because in new cases the patient does not present changes, and in cases with a higher age range the possibility of the occurrence of pulmonary changes will be increased. In Wuhan, China 2019, the mean age of patients was 47 years; 41.9% of patients were female. The most common symptoms were fever (43.8% on admission and 88.7% during hospitalization) and cough (67.8%). Diarrhea was infrequent (3.8). On admission, ground-glass opacity was the most common radiological finding on chest computed tomography (CT) (56.4%). No radiographic or CT abnormalities were found in 157 of 877 patients (17. 9%) with non-severe disease and in 5 of 173 patients (2.9%) with severe disease39.
As COVID-19 spreads to areas with large cosmopolitan populations, understanding how ethnicity affects COVID-19 outcomes is essential40. Blacks and ethnic minorities may be at higher risk for acquisition, disease severity, and poor outcomes on COVID-19 for several reasons. Specific ethnic groups, such as South Asians, have higher rates of some comorbidities, such as diabetes, hypertension, and cardiovascular disease, which have been associated with severe disease and mortality in COVID-1941. Ethnicity may interact with the spread of the virus through cultural, behavioral, and social differences, including lower socioeconomic status, health-seeking behavior, and intergenerational cohabitation40. We found significant differences in the number of reported contacts by age, gender, race, and ethnicity. Certain demographic groups, including people younger than 45, black and Hispanic men and respondents, have significantly higher contact rates than the rest of the population. Tracking changes in interpersonal contact patterns can provide rapid assessments of the impact of physical distancing policies during the course of the pandemic and help identify populations at risk42.
Knowledge of populations at higher risk of worsening and death from the disease is of utmost importance and is part of therapeutic strategies to prevent worsening of the disease in these populations43. In Distrito Federal, the prevalence of the Coronavirus disease varied from place to place, having its highest prevalence in Sobradinho with 12.82%28. The risk of contracting a directly transmitted infectious disease, such as Coronavirus Disease 2019 (COVID-19), depends on who interacts with whom. These person-to-person interactions vary by age and location-for example, at home, at work, at school, or in the community-due to different social structures. These social structures and contact patterns vary between and within countries. Although social contact patterns can be measured through surveys, most countries around the world, especially low and middle income countries, lack nationally representative contact surveys44.
There was good sensitivity and accuracy between CT scan and RT-PCR, highlighting that RT-PCR is difficult to perform, and that its detection rate is affected by several factors, such as sampling, storage, and reagent performance, and that in our reality this may have affected the results obtained, reducing this sensitivity obtained by the frequent occurrence of false negatives.
There was significant accuracy of CT scan in symptomatic patients suspected of COVID-19, highlighting that the sensitivity increases with age and in men, more prevalent in the pathology. Considering the prevalence, in low prevalence sites, normal CT scans almost rule out the pathology, whereas in high prevalence sites or situations, we have demonstrated that the presence of pulmonary alterations confirms the disease.
Conclusion
The sensitivity and accuracy of CT scan in relation to PCR-RT was significant. Sensitivity increases with prevalence and is more significant in the older age group and in men, who are more affected in this pathology.
Financing Source
None
References
- 1.Smith D L, Grenier J-P, Batte C, Spieler B.A Characteristic Chest. Radiographic Pattern in the Setting of COVID-19 Pandemic .
- 3.liu Wenzhong. (2020) hualan L. COVID-19: Attacks the 1-Beta Chain of Hemoglobin and Captures the Porphyrin to Inhibit Human Heme Metabolism.
- 4.Kampf G, Todt D, Pfaender S, Steinmann E. (2020) Persistence of coronaviruses on inanimate surfaces and their inactivation with biocidal agents. J Hosp Infect. 104(3), 246-251.
- 6.Ruiyun Li, Sen Pei, Bin Chen. (2020) Substantial undocumented infection facilitates the rapid dissemination of novel coronavirus (SARS-CoV2). Science. 3221, 1-9.
- 7.Strunk J L, Temesgen H, Andersen H, Packalen P. (2014) Imaging Profile of the COVID-19 Infection: Radiologic Findings and Literature Review Authors:. 80(2), 1-8.
- 8.Choi W, My T, Tran L. (2020) Performance of radiologists in differentiating COVID-19 from viral pneumonia on chest CT. , Radiology 1, 1-13.
- 9.Zhong L, Gong P, Biging G S. (2012) Clinical and Chest Radiography Features Determine Patient Outcomes In Young and. 78, 1-15.
- 10.Salehi S, Abedi A, Balakrishnan S, Gholamrezanezhad A. (2020) Coronavirus disease 2019 (COVID-19): A systematic review of imaging findings in 919 patients. , Am J Roentgenol 215(1), 87-93.
- 11.Vardhanabhuti V, Loader R J, Mitchell G R, Riordan R D, Roobottom C A. (2013) . , Cardiopulmonar y Imaging • Original Research. AJR Am 200-545.
- 12.Tay M Z, Poh C M, Rénia L. (2020) The trinity of COVID-19 immunity , inflammation and intervention. 2, 17-20.
- 13.Kooraki S, Hosseiny M, Myers L, Gholamrezanezhad A. (2020) Coronavirus (COVID-19) Outbreak: What the Department of Radiology Should Know. , J Am Coll Radiol 17(4), 447-451.
- 14.Hospital M, Chai Hospital Y. (2020) . Radiological Findings of 2019-nCoV Pneumonia PMH Experience .
- 15.Xiang Y, Yu D, Qin X, Li X, Zhang Q. (2020) Clinical and CT manifestations of coronavirus disease 2019. J Xi’an Jiaotong Univ Medical Sci. 41(4), 492-496.
- 16.Zhou S, Wang Y, Zhu T, Xia L. (2019) CT features of coronavirus disease. (COVID-19) pneumonia in 62 patients in 214(6), 1287-1294.
- 17.Strunk J L, Temesgen H, Andersen H, Packalen P. (2014) . Chest CT Findings in Coronavirus Disease-19 (COVID-19): Relationship to Duration of Infection 80(2), 1-8.
- 18.Radiologia SG De.Infectologia SG. Recomendações para Otimização da Solicitação e Leitura de TC do Tórax Pandemia COVID-19 Recomendações para Otimização da Solicitação e.
- 19.Song F, Shi N, Shan F. (2020) . Emerging 2019 novel coronavirus (2019-NCoV) pneumonia. Radiology 295(1), 210-217.
- 20.Zhao W, Zhong Z, Xie X, Yu Q, Liu J. (2020) Relation between chest CT findings and clinical conditions of coronavirus disease (covid-19) pneumonia: A multicenter study. , Am J Roentgenol 214(5), 1072-1077.
- 21.Strunk J L, Temesgen H, Andersen H, Packalen P. (2014) Radiology Department Preparedness for COVID-19: Radiology Scientific Expert Panel. 80(2), 1-8.
- 22.Li Y, Xia L. (2020) Coronavirus disease 2019 (COVID-19): Role of chest CT in diagnosis and management. , Am J Roentgenol 214(6), 1280-1286.
- 23.Ciccarese F, Coppola F, Spinelli D. (2020) Diagnostic Accuracy of North America Expert Consensus Statement on Reporting. CT Findings in Patients with Suspected COVID-19 Infection: An Italian Single Center Experience. Radiol Cardiothorac Imaging 2(4), 200312.
- 24.K De Smet, D, Ryckaert T. (2020) . Diagnostic Performance of Chest CT for SARS-CoV-2 Infection in Individuals with or without COVID-19 Symptoms. Radiology 202708.
- 25.Ai T, Yang Z, Xia L. (2020) . Correlation of Chest CT and RT-PCR Testing in Coronavirus Disease. Radiology 1-23.
- 26.Simpson S, Kay F U, Abbara S. (2020) Radiological Society of North America Expert Consensus Statement on Reporting Chest CT Findings Related to COVID-19. Endorsed by the Society of Thoracic Radiology, the American College of Radiology, and RSNA - Secondary Publication. J Thorac Imaging. 35(4), 219-227.
- 28.Ai T, Yang Z, Hou H. (2020) (COVID-19) in China: A Report of 1014 Cases. Correlation of Chest CT and RT-PCR Testing for Coronavirus Disease , Radiology 296(2), 32-40.
- 29.SP Meirelles G de. (2020) COVID-19 uma breve atualização para radiologistas. , Radiol Bras 53(5), 320-328.
- 30.Sardanelli F, G Di Leo. (2020) Assessing the value of diagnostic tests in the Coronavirus disease 2019 pandemic. , Radiology 296(3), 193-194.
- 31.Song F, Shi N, Shan F. (2020) . Emerging 2019 novel coronavirus (2019-NCoV) pneumonia. Radiology 295(1), 210-217.
- 32.Leeflang M M, Rutjes A W, Reitsma J B, Hooft L, Bossuyt P M. (2013) Variação da sensibilidade e especificidade de um teste com a prevalência da doença . , CMAJ 185(11), 537-544.
- 33.Leeflang M M, Bossuyt P M, Irwig L. (2009) A precisão do teste de diagnóstico pode variar com a prevalência: implicações para o diagnóstico baseado em evidências. , J Clin Epidemiol 62(1), 5-12.
- 34.Brent P Little, Jonathan H Chung, Brett M Elicker, Loren H Ketai. (2020) Essentials for Radiologists on COVID-19: An Update - Radiology Scientific Expert Panel. , Radiology 296(2).
- 35.Constantine A Raptis, Mark M Hammer, Ryan G Short, Shah Amar, Bhalla Sanjeev et al. (2020) Cardiopulmonary Imaging - Clinical Perspective. Chest CT and Coronavirus Disease (COVID-19): A Critical Review of the Literature to , Date, AJR 215(4).
- 36.MD David L Smith, John-Paul Grenier MD, Catherine Batte MS, Bradley Spieler MD. (2020) . A Characteristic Chest Radiographic Pattern in the Setting of COVID-19 Pandemic. Radiology: Cardiothoracic Imaging.2(5) .
- 37.CODEPLAN. (2020) Companhia de Planejamento do Distrito Federal. Governo do Distrito Federal. Boletim COVID-19 Nº 7 .
- 38.BARBOSA I R, MHR GALVÃO, SOUZA T A, GOMES. (2020) SM,MEDEIROS A DE A, LIMA KC. Incidência e mortalidade por covid-19 na população idosa brasileira e sua relação com indicadores contextuais: um estudo ecológico. Rev Bras Geriatr Gerontol. 23(1), 200171.
- 39.Bao C, Liu X, Zhang H, Li Y, Liu J. (2020) Coronavirus Disease 2019 (COVID-19) CT Findings: A Systematic Review and Meta-analysis.J Am CollRadiol. 17(6), 701-709.
- 40.Boehmer T, DeVies J, Caruso E. (2020) . Changing Age Distribution of the COVID-19 Pandemic —.MorbMortalWklyRep 69(39), 1404-1409.
- 41.Mistry D, Litvinova M, A Pastore y Piontti. (2021) Inferring high-resolution human mixing patterns for disease modeling.NatCommun. 12(1), 8-9.
- 42.Lavezzo E, Franchin E, Ciavarella C. (2020) Suppression of a SARS-CoV-2 outbreak in the Italian municipality of Vo’.Nature. 584(7821), 425-429.
- 43.Feehan D M, Mahmud A S. (2021) Quantifying population contact patterns in the United States during the COVID-19 pandemic.Nat Commun. 12(1), 893.
- 44.W J Guan, Z Y Ni, Hu Y, W H Liang, C Q Ou et al. (2020) . Clinical Characteristics of Coronavirus Disease in 382, 1708-1720.
- 45.(2020). Covid-19 National Emergency Response Center, E.; Case Management Team, K.C.F.D.C. Prevention. Early Epidemiological and Clinical Characteristics of 28 Cases of Coronavirus Disease in South Korea. Osong Public Health Res. Perspect 11, 8–14. .
- 46.. (2020). Center for Disease Control, U. Severe Outcomes among Patients with Coronavirus Disease Disease2019 (COVID-19)—United States, February 12- March 16, 2020. Morb. Mortal. Wkly. Rep. (MMWR) 69:, 343–346. .
- 47.Li R, Pei S, Chen B, Song Y, Zhang T et al. (2020) Substantial undocumented infection facilitates the rapid dissemination of novel coronavirus (SARS-CoV2). , Science 368, 489-493.
- 48.Gao J, Tian Z, X Breakthrough Yang. (2020) Chloroquine phosphate has shown apparent efficacy in treatment of COVID-19 associated pneumonia in clinical studies. , Biosci. Trends 14, 72-73.
- 49.Lee C. (2008) Raça” e “etnia” na pesquisa biomédica: como os cientistas constroem e explicam as diferenças na saúde? Soc Sci Med. 68, 1183-1190.
- 50.Zhao H, Harris R J, Ellis J, Pebody R G. (2015) Etnia, privação e mortalidade devido à pandemia de influenza A de2009 (H1N1) na Inglaterra durante a pandemia de 2009/2010 e a primeira temporada pós-pandêmica. Epidemiol Infect. 143, 3375-3383.
- 51.Pareek M, Bangash M N, Pareek N, Pan D, Sze S et al.Etnia e COVID - 19 : uma prioridade urgente de pesquisa em saúde pública.Lanceta. 2 de maio de 2020;. 395(10234), 1421-1422.
- 52.Tillin T, Hughes A D, Mayet J. (2013) The relationship between metabolic risk factors and incident cardiovascular disease in Europeans, South Asians, and African Caribbeans. , J Am Coll Cardiol 61, 1777-86.
- 53.Lai C C, Liu Y H, Wang C Y, Wang Y-H, Hsueh S-C et al. (2020) Asymptomatic carrier state, acute respiratory disease, and pneumonia due to severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2): Facts and myths. , J Microbiol Immunol Infect 53(3), 404-12.
- 54.Li L-Q, Huang T, Wang Y-Q, Wang Z-P, Liang Y et al. (2020) Covid-19 patients’ clinical characteristics, discharge rate, and fatality rate of meta-analysis. , J Med Virol 92(6), 577-83.