
Abstract
The aim was to record the smoking behaviour of 13- to 16-year-old Austrian pupils and to investigate changes in smoking behaviour following amendments of legislation and gender-specific differences.
The survey took place in Vienna, Lower Austria, Burgenland, Styria and Carinthia and was conducted at eight different school types. The data was collected by means of a questionnaire in a group setting at the beginning of a school lesson. The completion of the questionnaire was anonymous. 95,1% of the returned questionnaires could be used for this study, yielding data from a total of 1029 young people for analysis.
38.4% of the participants stated that they had at least once consumed tobacco or related products, with girls having tried them more often (41,6%) than boys (34,9%) (p = .028). At the time of the study, 3,3% used tobacco daily and 4,6% several times a week; thus 7,9% smoke regularly. Although friends or family are the most popular type of acquisition for girls and boys, girls buy their tobacco products from vending machines (11,6%) much more frequently than boys (6,0%) (p = .014) and prefer normal cigarettes (p < .001).
The results of this study show that while the number of adolescents who smoke daily is decreasing, the number of occasional smokers is increasing. Already 38,4% of the 13 to 16-year olds have had some experience consuming tobacco. Austria must take the measures recommended by the WHO to reduce the smoking prevalence and protect minors from the health damage caused by tobacco smoke.
Author Contributions
Academic Editor: Qiang Cheng, Biomedical Informatics Institute, and CompAuter Science Department, China.
Checked for plagiarism: Yes
Review by: Single-blind
Copyright © 2020 Julia Berger ,et al.
 This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Competing interests
The authors have declared that no competing interests exist.
Citation:
Introduction
About 1.1 billion people smoke worldwide and more than eight million people die every year as a result of tobacco consumption - of which about 1.2 million die as non-smokers as a result of passive smoking. From a medical point of view, tobacco is responsible for the biggest public health crisis that mankind has to deal with.1 Smoking behaviour is greatly influenced by the close environment, especially family and friends, the availability and cost of tobacco and related products, and individual curiosity. Most nicotine addicts start smoking before the age of 20.2 Children and teenagers who start smoking develop a tobacco addiction especially fast. As many as 10% of them show signs of addiction after using it for more than two days and another 50% if they smoke at least seven cigarettes a month.3
Tobacco consumption in childhood influences the current state of health of the child and carries the risk of long-term health damage. The short-term consequences of childhood tobacco use include reduced physical performance, nicotine dependence and can lead to asthma and other lung diseases.4 Minors who regularly consume tobacco are also more likely to be diagnosed with anxiety and/or mood disorders. Children who smoke are also said to have a lower inhibition threshold to alcohol or illegal drugs.5 Because of the early exposure of the child’s body to the toxins of tobacco smoke, the risk of cardiovascular disease, malignant neoplasia and respiratory tract diseases is even higher than for adult smokers. In 2015, around a quarter of 15 to 16-year olds in Europe reported having smoked in the last month. In the year of the 16th birthday of Austrian pupils, a lifetime prevalence of tobacco consumption of 53% (EU average 46%) and a 30-day prevalence of 28% (EU average 21%) was reported.6
Children and adolescents are often passively exposed and easily influenced by advertising without being aware of it nor being able to protect themselves. Lifelong non-smokers who were exposed to tobacco smoke either in childhood or later by their partner or at work are up to two times more likely to develop lung cancer. If at least one parent smokes in the presence of a child, the likelihood of asthma, other respiratory diseases such as pneumonia or bronchitis, otitis media and meningitis for the child increases. In addition, these children have the double risk of becoming nicotine dependent in the future, since they not only inhale the addictive smoke but also mimic the behavioural pattern of smoking. Infants whose mothers smoke, have an increased risk of dying of “sudden infant death syndrome” (SIDS) in the first year of life.7 Smoking bans at work including restaurants and bars did not only reduce exposure and respiratory disease of employees, but also cardiovascular disease in the general population and they raised awareness about dangers of second-hand smoke (SHS) for children and pregnant women, leading to a decrease of SHS in homes and cars and to a reduction of premature birth by 4% and of hospital admissions for children diagnosed with asthma by 10% or with lower respiratory infections by 19%. Children should be considered the most important target group for non-smoker protection and smoking prevention.8, 9, 10
The Austrian government signed the Framework Convention on Tobacco Control (FCTC) in 2005 but has taken time to implement the regulations.11 On January 1st 2019, the age limit for the possession, purchase and consumption of tobacco and related products has been raised from 16 to 18 years throughout Austria.12 In comparison, the age limit was raised way earlier in many other EU countries, e.g. in Germany already in 2007.13 The Protection of Young Persons Acts in the 9 federal provinces of Austria have been aligned, but still differ significantly in some points. In Lower Austria, Vienna, Tyrol and Burgenland, the ban is limited to public spaces only, while in the other provinces a general ban applies.14, 15, 16, 17, 18, 19 The last study concerning the smoking behaviour of Austrian school children was conducted 2017/18, before the age limit was raised.20 Since November 1st 2019, the smoking ban in Austria finally also applies in rooms for the production, processing, administration or consumption of food or beverages and in gastronomy establishments for all areas available to guests, with the exception of open-air areas. Except for outdoor areas of restaurants and bars the Austrian hospitality industry is now smoke-free.21 This contributed to the significant improvement of Austria’s tobacco control ranked by the European Cancer League in 2020. (https://www.tobaccocontrolscale.org/TCS2019.pdf).
Methods and Materials
The participants were pupils at Austrian schools who were aged between 13 and 16 years at the time of the study. The Ethics Committee of the Medical University of Vienna has given a positive vote on 26 August 2019 under EC No. 1736/2019 for the implementation of the present study. In the federal provinces of Lower Austria, Burgenland, Carinthia and Styria, permission to conduct the study was obtained from the respective provincial school boards. Subsequently, the request was sent to the directorates of the selected schools. In Vienna, the City School Board referred directly to the relevant school institutions. The survey was conducted by means of a questionnaire based on the Health Behaviour in School-aged Children (HBSC) and the Eurobarometer questionnaire.20, 22 The survey was conducted at the beginning of lessons in classes of the participating schools. At first a description of our project was given, and the students were instructed and informed about the anonymity of the survey and the voluntary nature of participation, which was also written down for the pupils to read on the first page of the questionnaire. After filling out the questionnaires in a group setting, the questionnaires were collected by a student and placed in an envelope. The questions were divided into three categories: General & Social, Smoking Behaviour and Health Awareness.
The data collected was first entered into a corresponding Microsoft Excel Office 365 database, with continuous monitoring of the correctness of the entries. This data set was then transformed into an SPSS data matrix. Inferential and descriptive statistical analyses were performed using IBM SPSS® 26 for Windows statistical software. The significance level was pre-set to α = 5%, according to the probability of error, so a result in inferential statistics with p ≤ .05 is considered significant. For descriptive statistics, the mainly categorical variables were given by means of absolute and relative frequencies, the age of the participants (as the only metric variable) with their mean and standard deviation. Confidence intervals have been calculated to give a range estimate for unit values.
To test correlations, the Chi-square test was used based on cross tables for the categories of nominally scaled variables. This enables a comparison of theoretical and empirical distributions. Thus, for a given association between two variables, the test variable χ2 can be used to check whether the observed frequencies of combinations of characteristics differ significantly from expected frequencies, considering the degrees of freedom (df). In this case, a distribution difference can be assumed. For at least ordinally scaled data, the Mann-Whitney U-test was used as an alternative procedure instead of the t-test for independent samples with restrictions of the normal distribution assumption as the method of choice.23
The answers of the questionnaire were coded, and variable sets were created for the questions with optional multiple-choice answers. For a better overview, the study population was divided into four groups according to their smoking behaviour. Question 2.1 "Have you ever smoked tobacco?" and question 2.8 "How often do you smoke at the moment?”. The group "never smoker" answered question 2.1. with "No", the group " try smoker" answered question 2.1. with "Yes" and question 2.8. with "I do not smoke (anymore)", the group "occasional smoker" answered question 2.1. with "Yes" and question 2.8. with "less than once a week" or "several times a week" and the group "daily smoker" answered question 2.1. with "Yes" and question 2.8. with "daily". "Try smokers" have already consumed tobacco once in their lifetime but no longer smoke at the time of the survey, "occasional smokers" smoke irregularly or not every day, while "daily smokers" consume tobacco daily.
Results
Of the total of 1082 questionnaires submitted, 1029 could finally be evaluated, resulting in a proportion of 95,1%, with a drop-out rate of 4,9%.
Descriptive Statistics
Of the 1029 participants, 531 (51,6%) were female and 498 (48,4%) male. The calculation of a corresponding Chi-square test to check for equal distribution was not significant with χ2(1) = 1,058, p = .304, so that the percentages were comparable regarding the gender of the participants. The mean age (n=1029) at the time of the survey was 14.76 ± 1.01 (min 13, max 16) years, the corresponding median age was 15 years. The average age of the girls was 14.89 ± .99 years, that of the boys 14.62 ± 1.01 years, so that the examination of the difference with z = -4.314, p < .001 by U-test also indicated a slightly higher age of the girls.
Concluding Statistics
(At least) Single Use of Tobacco
In total, 395 (38,4%; 95% confidence range (35,4%; 41,4%)) of the girls and boys stated that they had used tobacco at least once in their lives. Of the 531 girls, 221 (41,6%, (37,4%; 45,8%)) have already used tobacco and 310 (58,4%) have never used it. Of the 498 boys, 174 (34,9%, (30,8%; 39,1%)) have at least once used tobacco and 324 (65,1%) have never used it (Figure 1). Data analysis using Pearson's Chi-square test showed a significant relationship between tobacco use and gender, with χ2(1) = 4.848, p = .028. The corresponding test values showed within the genders for both girls with χ2 (3) = 4.142, p = .370 and for boys with χ2(3) = 2.607, p = .456 a non-significant distributional difference regarding a change with age groups, which means the experience did not increase significantly with higher age groups and the more frequent tobacco try-out among girls cannot be attributed to their slightly higher age (compared with boys).
Figure 1.Percentage of at least one-time experience of tobacco use in relation to age groups, regarding gender (with polynomial trend lines)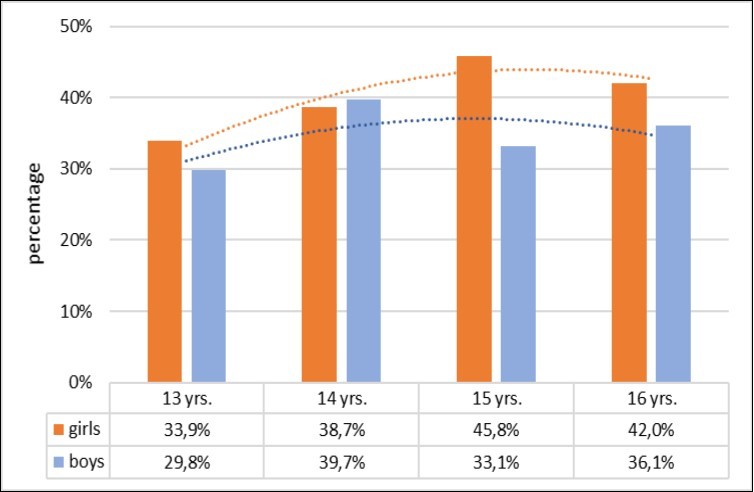
Smoking Behaviour (Four Categories)
Out of the 1029 participants 995 (96,7%) could be divided into four categories ("never-smoker", "try-smoker", "occasional smoker" and "daily smoker"). The group of "never-smokers" is clearly the largest with 634 (61,6%; (58,9%; 64,0%)) participants, 310 (58,4%; (54,0%, 62,9%)) girls and 324 (65,1%; (61,0%, 69,3%)) boys. 223 (21,7%; (19,2%; 24,4%)) of the pupils classify as "try smokers", 124 (23,4%; (20,0%, 27,1%)) girls and 99 (19,9%; (16,5%, 23,7%)) boys. “Occasional smokers" include 104 (10,1%, (8,4%, 12,0%)) pupils, 56 (10,5%, (8,5%; 12,8%)) girls and 48 (9,6% (7,4%; 11,8%)) boys. The smallest group are the "daily smokers", with 34 (3,3%, (2,3%; 4,4%)) adolescents, of whom 16 (3,0%, (1,9%, 4,1%)) are female and 18 (3,6%, (2,4%; 5,0%)) male (Table 1).
Table 1. Equity value with expected values and standardised residuals of the four categories of smoking behaviour regarding the gender, n=1029| Gender | Smoker categories | ||||
| never | try | occasional | daily | ||
| Female | qty. (expected qty.; stand. res.) | 310 (327.2; -0.9) | 124 (115.1; 0.8) | 56 (53.7; 0.3) | 16 (17.5; -0.4) |
| equity value | 58,4% | 23,4% | 10,5% | 3,0% | |
| Male | qty. (expected qty.; stand. res.) | 324 (306.8; 1.0) | 99 (107.9; -0.9) | 48 (50.3; -0.3) | 18 (16.5; 0.4) |
| equity value | 65,1% | 19,9% | 9,6% | 3,6% | |
The corresponding test values showed within the genders for both girls with χ2(9) = 4.538, p = .873 and for boys with χ2(9) = 13.587, p = .138 a non-significant distribution difference regarding a change with the age groups, i.e. the allocation to the different groups does not change significant with higher age groups.
Type of Acquisition
Multiple-choice was possible regarding the question about the type of acquisition of tobacco products for minors. The possible answers were tobacco shop, vending machine, friends, internet, family and others. The question was answered by 152 (56,7%) girls and 116 (43,3%) boys. Friends are the most common source of tobacco for both sexes: 120 (78,9%) girls and 76 (65,5%) boys. Tobacco shops and cigarette vending machines are used equally frequently by girls, with 31 (20,4%) each and a total of 62 (40,8%). Among boys, the tobacco shops are more popular as a source of tobacco with 35 (30,2%) responses compared to the vending machine with 16 (13,8%). 33 (21,7%) girls (also) get their tobacco products from family members versus 21 (18,1%) among the boys. The Internet as a place of purchase plays a greater role for boys than for girls (9 (7,8%) boys versus 5 (3,3%) girls). Using the chi-square test, a significant relationship between gender and type of acquisition of tobacco products was found (p = .014). The gender-specific difference regarding using the cigarette vending machines should be emphasised (Table 2). Girls use this reference option significantly more often than boys (Chi-square test, p = .044).
Table 2. Equity values with expected values and standardized corrected residuals to the tobacco source vending machine as well as percentages (line percentages per gender)| Gender | Vending machines | Total | ||
| No | Yes | |||
| Female | qty. (expected qty.; stand. corr. res.) | 500 (506.7; -2.0) | 31 (24.3; 2.0) | 531 |
| equity value | 94,2% | 5,8% | 100,0% | |
| Male | qty. (expected qty.; stand. corr. res.) | 482 (475.3; 2.0) | 16 (22.7; -2.0) | 498 |
| equity value | 96,8% | 3,2% | 100,0% | |
| Total | quantity (equity value) | 982 (95,4%) | 47 (4,6%) | 1029 |
Mode of Consumption
The question about the mode of consumption was answered by 364 (35,4%) of the 1029 pupils. Only the 395 participants who had already consumed tobacco at least once could give a valid answer to the question (364 corresponds to 92,2%). Multiple-choice answers were possible. The possible responses were regular cigarettes, hand-rolled cigarettes, e-cigarettes, flavoured cigarettes, water pipe (shisha), oral tobacco, cigar/pipe and others. Of the 364 pupils who answered this question, 70,6% have consumed tobacco through regular cigarettes, 49,2% smoked water pipe, 38,5% e-cigarette, 20,1% flavoured cigarettes, 15,1% hand-rolled cigarettes and 12,1% cigar or pipe. 11,0% consumed oral tobacco.
Of the 364 young people, 204 (56,0%) were girls and 160 (44,0%) boys. Regular cigarettes were consumed by 157 (77,0%) of the girls and 100 (62,5%) of the boys, water pipe by 93 (45,6%) of the girls and 86 (53,8%) of the boys, e-cigarettes by 69 (33,8%) of the girls and 71 (44,4%) of the boys, flavoured cigarettes by 44 (21,6%) of girls and 29 (18,1%) of boys, hand-rolled cigarettes by 23 (11,3%) of girls and 32 (20,0%) of boys and cigar or pipe by 20 (9,8%) of girls and 24 (15,0%) of boys. Oral tobacco was consumed by 15 (7,4%) of girls and 25 (15,6%) of boys. A significant dependence of the mode of consumption on gender was demonstrated by means of the Chi-square test (p < .001). Girls preferred regular cigarettes, while boys were significantly more likely to consume hand-rolled cigarettes, e-cigarettes and oral tobacco than girls. Although the water pipe is slightly more popular among boys (23,4%) than among girls (22,1%), it was the second most popular form of tobacco consumption for both sexes. Out of 14 participants who stated that they buy their tobacco products (among others) on the Internet, 12 (85,7%) consumed e-cigarettes. There is a significant relationship between the place of purchase and the consumption of e-cigarettes (Chi-square test, p = .011).
Discussion
Smoking Behaviour
The latest study (HBSC) about the smoking behaviour of Austrians pupils 2017/18 was conducted before the legal age limit for tobacco in Austria was raised to 18 years. The number of daily smokers among pupils sank from 2017/18 to 2019: While 3,9% of the girls and 5,0% of the boys smoked daily in the HBSC study, only 3,0% (1,9%; 4,3%) of the girls and 3,6% (2,2%; 5,0%) of the boys did in this study 2019. However, the number of occasional smokers has increased significantly. In the 2017/18 HBSC survey, 8,8% of girls and 6,2% of boys stated that they consumed tobacco occasionally. In the present study, 10,5% ((8,5%; 12,8%)) of girls and 9,6% ((7,4%; 11,8%)) of boys stated to do so. This may also be due to the fact that, compared to the HBSC study (24,0% girls and 19,2% boys), many more pupils stated that they had already used tobacco at least once (41,6% (37,4%; 45,8%) girls and 34,9% (30,8%; 39,1%) boys). The comparison also shows that the younger age group in particular has had more frequent experience with tobacco in the present study.20 This is worrying and calls for a more detailed investigation of birth cohorts.
Type of Acquisition
Following the increase of the minimum age for the sale of tobacco products to 18 years at the beginning of 2019, the present study showed the following results among the participants who already had smoked: Friends are the most popular source of tobacco for minors (73,1%). However, tobacco shops are still frequently used as a source of supply for minors (24,6%) as well as vending machines (17,5%). A significant gender-specific difference could be observed: 20,4% of the girls stated that they used vending machines, while only 13,8% of the boys did. It has been shown that electronic age verification cards at vending machines are not a complete protection for minors and that young people easily regain access to tobacco products by borrowing these cards from friends or family members.24 Vending machines are also used for tobacco advertising, often deliberately in front of schools and on school routes. Further it is important that the age of a customer of a tobacco shop must be checked, as it is prohibited to sell tobacco to minors, but obviously is still possible for children to get tobacco products through these shops. In 2014 the first mystery shopping was conducted in Upper Austria: A total of 98 businesses were tested, but 59,2% of them failed and sold cigarettes to people under 16 years of age.25 In Styria 400 businesses selling alcohol and/or tobacco products were tested in 2016. Only about 60% of the outlets asked for the identification of 14-15-year-old test buyers, refused to sell and thus complied with the law on the protection of minors.26 These results clearly show that age control by the tobacco monopoly administration failed and that an independent institute should be commissioned to perform mystery shopping in all 9 Austrian provinces. In addition advertising and display of tobacco products need to be banned in shops providing goods for children like cartoons, soft-drinks, sweets or toys. Tobacconists who want to display tobacco products should be allowed to do this only indoors if access to minors is prevented like in Hungary. Display bans must not be circumvented by transparent walls. Because electronic age control is unreliable and vending machines are used for outdoor advertising, all vending machines for cigarettes should be banned.
Mode of Consumption
In the latest Austrian HBSC study, 8,7% of 13-year-old girls and 11,5% of 13-year-old boys, as well as 32,1% of 15-year-old girls and 33,0% of 15-year-old boys stated, that they had consumed normal cigarettes, regardless of the frequency of consumption.20 Of the 13-year-old girls in this study, 27,1% have already had experience with regular cigarettes and 16,7% of 13-year-old boys. Among the 15-year-old participants, 30,5% of the girls and 17,1% of the boys have already consumed normal cigarettes at least once. While the normal cigarette is much more popular in the present study, especially among younger students, the situation is different with the shisha. In the Austrian HBSC study, only students aged 15 and over were asked about their consumption of shisha and e-cigarette. 33,1% of the 15-year-old girls and 40,4% of the 15-year-old boys stated that they had smoked shisha before, while in the present study only 22,0% of the 15-year-old girls and 20,6% of the 15-year-old boys did. After the ban of smoking went into force on November 1st, 2019, shisha venues had to close, where some adolescents had their first tobacco experience under group pressure. For some this had been the first deep inhalation of tobacco smoke resulting in nicotine flooding of the brain. Therefore it was important to reduce this possible gateway to nicotine addiction.
Also with regard to e-cigarettes the trend seems promising: Among 15-year-old girls, 31,1% stated in the latest Austrian HBSC study that they had consumed e-cigarettes at least once, among boys it was already 44,1%. In comparison, 14,8% of the 15-year-old participants in the present study tried e-cigarettes: 15,8% of the girls and 13,7% of the boys.20 With regard to the higher proportion of e-cigarette consumption in the HBSC study, it should be noted that the survey was conducted prior to the publication of acute lung damage in the U.S. from e-cigarettes. During the present study, media had already reported on "EVALI" (“e-cigarette or vaping product use associated lung injury”) among adolescents.27 Nevertheless continuation of monitoring use of e-cigarettes and other nicotine products by minors is necessary. Internet access of minors to cigarettes should be prevented by increase of customs checks, sham orders, etc.
Limitation
The study was conducted by means of a questionnaire, so the results depend on the honesty of the participants. It is possible that participants have chosen the more socially acceptable answer options and therefore the results do not completely correspond to reality. As it was carried out in only five provinces, the study cannot be considered representative for Austria.
Conclusion
In general, the trend of daily smokers in Austria is moving in the right direction in terms of health policy. The year 2019 brought significant legal changes in Austria: The age limit for the purchase of tobacco products and related products was raised to 18 years and smoking in restaurants and bars was prohibited. However, the legal possibilities for reducing the smoking rate in Austria are far from exhausted. Further improvements are necessary to reduce the smoking prevalence and, above all, to discourage minors from smoking. The focus of tobacco prevention should shift now to a reduction of tobacco retailers, who should lose their license for selling tobacco and nicotine products after repeated neglect of age control.
Acknowledgements
We thank the pupils of selected schools for their high participation rate, parents, teachers, school directors and school boards for permission of the investigation, Isabella Heißenberger, Elena Fakia and Felix Rick for their help to prepare the study and collect the data.
References
- 1.WHO.Tobacco Fact Sheet [Internet]. [cited2019Sep3]. p. 1–9. Available from: https://www.who.int/news-room/fact-sheets/detail/tobacco
- 2.Lichtenschopf A. (2012) Standards der Tabakentwöhnung, Konsensus der Österreichischen Gesellschaft für Pneumologie -. Update2010. Wien:Springer-Verlag;
- 3.Van Schayck OCP, Williams S, Barchilon V, Baxter N, Jawad M et al.Treating tobacco dependence: guidance for primary care on life-saving interventions. Position statement of the IPCRG. npj Prim Care Respir Med.
- 4.(2018). OECD Health Division. Health at a Glance: Europe2018[Internet]. OECD;2018[cited2019Jun 25].216 p. (Health at a Glance: Europe)..
- 5. (2016) Health at a Glance: Europe. (Health at a Glance: Europe). Available from: https://www.oecd-ilibrary.org/social-issues-migration-health/health-at-a-glance-europe-2016_9789264265592-en , [Internet]. OECD;
- 6. (2016) . ESPAD Group. ESPAD Report2015:Results from the Europeam School Survey Project on Alcohol and Other Drugs [Internet]. Publications Office of the European Union, Luxembourg;104 p .
- 7.Burger R, Davani K. (2017) Schwarzbuch Zigarette: Rauchen gefährdet ihr. Bewusstsein. 2. Auflage , Wien; 300.
- 8.Neuberger M. (2019) Positive Auswirkungen einer restriktiven Tabakpolitik. J.Pneumolog. 7(2), 11-15.
- 9.Neuberger M. (2019) Effects of Involuntary Smoking and Vaping on the Cardiovascular System. , Int J Occup Environ Med 1(1), 10-18.
- 11. (2005) World Health Organization. WHO Framework Convention on Tobacco Control [Internet]. [cited 2019Nov26]
- 12. (2019) Rechtsinforamtionssystem des Bundes. Bundesrecht konsolidiert: Gesamte Rechtsvorschrift für Tabak - und Nichtraucherinnen - bzw. Nichtraucherschutzgesetz, Fassung vom 26.10.2019 [Internet].[cited2019Oct26].p.1–.
- 13.Kuntz B, Lampert T.Smoking and Passive Smoke Exposure Among Adolescents in Germany. Dtsch Aerzteblatt Online [Internet].2016Jan22;23–30. Available from: https://www.aerzteblatt.de/10.3238/arztebl.2016.0023.
- 14. (2019) Rechts inforamtions system des Bundes. Gesamte Rechtsvorschrift für NÖ Jugendgesetz. , Fassungvom08.11.2019[Internet].[cited2019Nov8]
- 15. (2019) Rechts inforamtion ssystem des Bundes. Gesamte Rechtsvorschrift für Burgenländisches Jugendschutzgesetz2002,Fassung vom08.11.2019[Internet].[cited2019Nov8.
- 16. (2019) Rechts inforamtions system des Bundes. Gesamte Rechtsvorschrift für Wiener Jugendschutzgesetz2002,Fassung vom08.11.2019[Internet][cited2019Nov8].
- 17. (2019) Rechts inforamtions system des Bundes. Landesrecht konsolidiert Tirol: Gesamte Rechtsvorschrift für Jugendgesetz, Tiroler, Fassung vom10.11.2019[Internet].[cited2019Nov10.
- 18. (2019) Rechts inforamtions system des Bundes. Landesrecht konsolidiert Oberösterreich: Gesamte Rechtsvorschrift für Oö. Jugendschutzgesetz2001,Fassung vom10.11.2019[Internet].[cited 2019Nov10].
- 19. (2019) Rechts inforamtions system des Bundes. Landesrecht konsolidiert Salzburg: Gesamte Rechtsvorschrift für Salzburger Jugendgesetz, Fassung vom10.11.2019[Internet].[cited2019Nov10].
- 20.Felder-Puig R, Teutsch F, Ramelow D, Maier G.. Gesundheit und Gesundheitsverhalten von österreichischen Schülerinnen und Schülern, Ergebnisse des WHO-HBSC-Survey2018 [Internet]. Wien: Bundesministerium für Arbeit, Soziales, Gesundheit und Konsumentenschutz (BMASGK);Available .
- 21. (2019) Rechts inforamtions system des Bundes. Bundesrecht konsolidiert: Gesamte Rechtsvorschrift für Tabak. und Nichtraucherinnen - bzw. Nichtraucherschutzgesetz, Fassung vom06.11.2019 [Internet].[cited2019Nov6].p.1– .
- 22. (2015) . European Commission. Special Eurobarometer 429: Attitudes of Europeans towards Tobacco and Electronic .
- 23.Weiß C. (2013) . , Basiswissen Medizinische Statistik[Internet].Berlin,Heidelberg:SpringerBerlin Heidelberg(Springer-Lehrbuch). 259-273.
- 24.Kanda H, Osaki Y, Ohida T, Kaneita Y, Munezawa T. (2011) Age verification cards fail to fully prevent minors from accessing tobacco products. , Tob Control 20(2), 163-5.
- 25. (2015) . Amt der Oö. Landesregierung. Testkäufe nach dem OÖ. Jugendschutzgesetz – Bilanz2014.Linz .
Cited by (4)
- 1.Neuberger Manfred, 2021, , , (), 1127, 10.1007/978-3-030-57499-4_124
- 2.Neuberger Manfred, 2021, , , (), 1, 10.1007/978-3-642-36206-4_124-1
- 3.Berger J., Neuberger M., 2020, Wer schützt Österreichs Kinder und Jugendliche vor Tabakindustrie und -handel?, Pädiatrie & Pädologie, 55(5), 248, 10.1007/s00608-020-00813-1
- 4.Vlachou Christina, Vejdovszky Katharina, Wolf Josef, Steinwider Johann, Fuchs Klemens, et al, 2021, Toxicological approaches for the quantitative inhalation risk assessment of toxic metals from tobacco smoke: application on the deterministic and probabilistic inhalation risk assessment of cadmium for Austrian smokers, Inhalation Toxicology, 33(4), 128, 10.1080/08958378.2021.1912859