
Abstract
Open bite malocclusion, due to it’s multifactorial etiology, has always been considered a difficult problem to treat. Often associated with transverse maxillary deficiency, this is a real challenge in the field of orthodontics. The traditional approach, for this type of anomaly, in adult patients, is orthognathic surgery and RME (rapid maxillary expansion). There are several approaches to the treatment of adult patients using digital technology. Mini-implant supported palatal expander limits the side effects of the conventional RME and is less invasive compared to orthognathic surgery. Precise and predictable mini-implant insertion, using a customized surgical guide, provides a safe therapeutic approach. This case report combines Cone-beam computed tomography (CBCT), laser scan superimposition, computer-aided design (CAD) and 3D printing in order to design and print a customized surgical guide for orthodontic mini-implant insertion. A CBCT scan was performed to determine the optimal site for mini-implants’ placement. Using the 3Shape Trios Intraoral Scanner the maxilla and the mandible were laser-scanned. Blue Sky Plan 4 software was used to design the surgical guide, and RayWare software was used for printing it. 4 mini-implants were inserted using a safe and predictable technique. The 3D technology represents the future of orthodontics, reducing the risks, chair-side time while providing the best treatment plan for the patient.
Author Contributions
Academic Editor: Sasho Stoleski, Institute of Occupational Health of R. Macedonia, WHO CC and Ga2len CC, Macedonia.
Checked for plagiarism: Yes
Review by: Single-blind
Copyright © 2020 Szuhanek C, et al.
 This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Competing interests
The authors have declared that no competing interests exist.
Citation:
Introduction
Open bite is an anomaly with distinct characteristics that can be easily recognized in 25 to 38 % of the orthodontic patients 1. Several etiological factors are responsible for this type of malocclusion such as: facial growth pattern, sucking habits, tongue-thrusting, mouth breathing, adenoid hypertrophy, syndromes, occlusal and eruptive forces, dental ankylosis, and postural mandibular imbalance. 2 Open bite is often associated with transverse maxillary deficiency, one of the most common malocclusions in orthodontics. 3
Rapid maxillary expansion (RME) is the treatment of choice for the transverse maxillary deficiencies and it is achieved through the remodeling of the midpalatal and inter-maxillary sutures, in children and teenagers. 4, 5
Due to the increased inter-digitation of the maxillary sutures and the rigidity of adjacent structures, the prognosis is not that favorable for adult patients. 6 Root resorptions,damage to periodontal tissues,7, 8, 9 technique failure or limitations,10 reduced stability, 11 edemas and soft tissue lesions 12 have been reported as side effects for adult patients.
In order to minimize the side effects of classical RME and to optimize the potential for skeletal expansion in adult patients Lee et al proposed a mini-screw assisted rapid palatal expansion (MARPE) appliance. 13 Mini-screw insertion site is critical and requires careful consideration of the hard and soft tissue, biomechanics, accessibility and patients’s comfort.
Digital technology plays a major role in contemporary orthodontics, changing the rules of conventional workflow. 14, 15, 16, 17, 18 Every procedure, from diagnosis and treatment outcome pre-visualization to the customization of the appliance design and customization of the therapy, is more predictable. 19, 20. The use of cone beam computer tomography (CBCT) allows for a more detailed diagnosis and selection for an insertion site with adequate bone quantity and quality. The placement of orthodontic mini-implants with a 3D method based on CBCT imaging has been described in recent years. 21, 22.
Materials & Methods
This study presents the 3D planning for a surgical guide in order to place a mini-implant supported maxillary expander.
In the case presented below, a male patient aged 25 years, with the chief complaint of posterior, skeletal, bilateral cross-bite and anterior open bite, was referred for orthodontic treatment. A rapid palatal expansion appliance was proposed using a skeletal expander anchored on 4 BENEfit® mini-implants.
A CBCT scan was performed to determine the optimal site for mini-implants’ placement. Using the 3Shape Trios Intraoral Scanner the maxilla and the mandible were laser-scanned (Figure 1). Blue Sky Plan 4 software was used to design the surgical guide, and RayWare software was used for printing it.
Figure 1.Digital models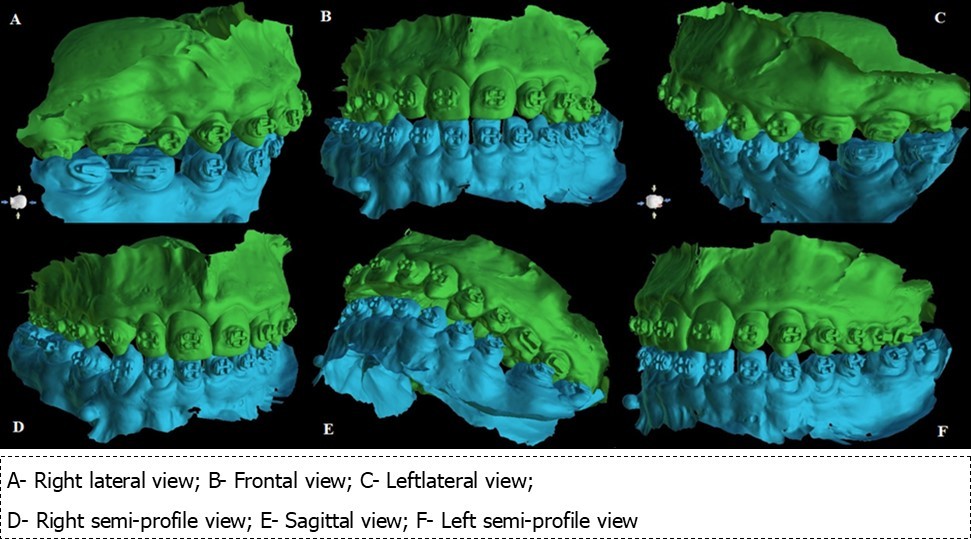
The digital model (stereolitography (STL) files) was superimposed on the CBCT scan (DICOM file (Digital Imaging and Communication in Medicine) file in order to facilitate the optimal positioning of the 4 mini-implants in the anterior hard palate.
Results
The most suitable antero-posterior mini-implant placement site is determined based on the width and thickness of the palatal vault. 4 self-drilling mini-implants (BENEfit®) were selected: 2 in the anterior palate (rugae area): 2.0 x 9 mm (ST-33-54209) and 2 in the posterior palate (para-midsagittal area): 2.0 x 7 mm (ST-33-54207). (Figure 2)
Figure 2.Mini-implant characteristics
The precise position and angulation of the mini-implants is replicated by 4 cylindrical metallic guides taking into consideration the following parameters: bone thickness, soft tissue thickness and anatomical surrounding structures. The most appropriate site for the placement of mini-implants is: 3 mm lateral to the suture in the first premolar region. (Figure 3,Figure 4)
Figure 3.Positioning of the 4 mini-implants, visualized on the basis of the intraoral scan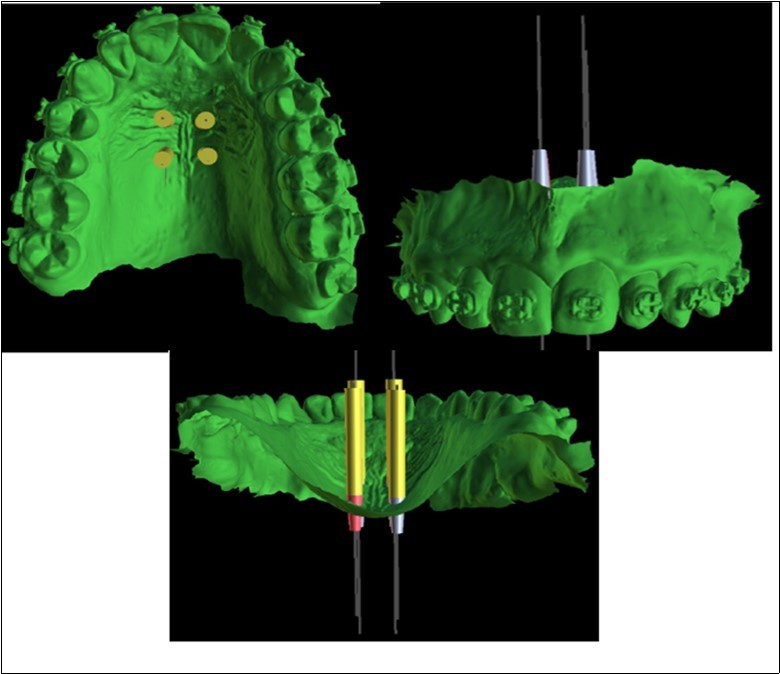
Figure 4.Positioning of the mini-implants on CBCT, A. Sagittal section, B. Coronal section, C. Axial section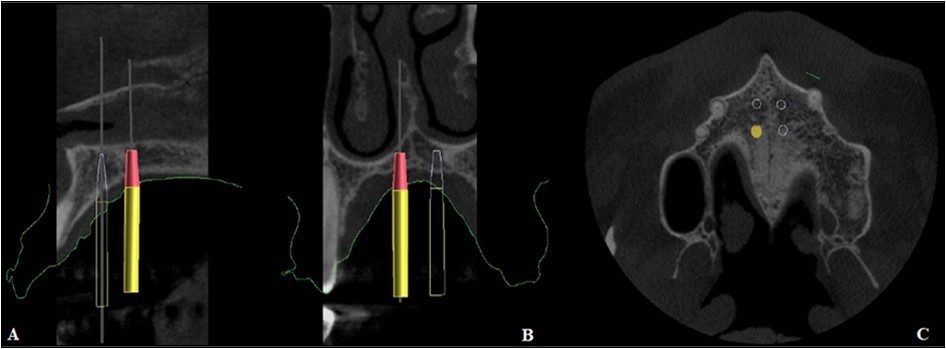
A 3D positioning guide was designed on top of the virtual model with the final mini-implant position. (Figure 5)
Figure 5.Designing the surgical guide
The customized surgical template was 1.8 mm thick layer offset based on the teeth/mucosa/ bracket contour profiles and ranged from incisors to second premolar. The surgical template was designed to cover the entire occlusal surface. (Figure 6)
Figure 6.Custom made surgical guide with mini-implant analogs final design
Patient’s initials are engraved on the outer surface of the guide, as well as the dimensions of the mini-implants in order to provide more safety and not cause confusion during the transfer from the printing office to the dental office (Figure 6).
After this stage, this file was exported in RayWare software (Figure 7) and printed using a autoclavable resin (Surgical Guide-MoonRay).
Figure 7.Final preview of the surgical guide before printing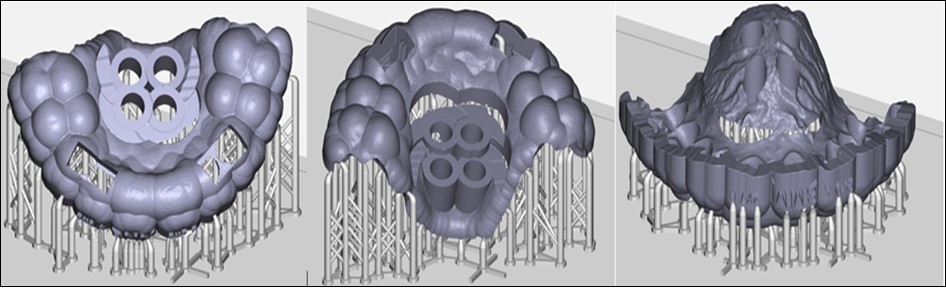
Discussion
The digital workflow in orthodontics consists of a triad of digital models, orthodontic software and 3D printers and allows for faster digital case planning, improving communication between professionals and patients without the use of physical documents. In addition, the accessibility and ease of use of this technology enables its wide use in diagnostic and treatment planning. 23, 24 Three-dimensional image processing allows for virtual planning using CAD (computer-aided design) software as well as CAM (computer-aided manufacturing), such as for the manufacture of surgical guides that were originally used in implantology. 25, 26. It is recommended to combine the knowledge of basic sciences and the evolution of new technologies in order to establish safer therapeutic approaches. 27
Software-based digital orthodontic planning allows the simulation of the mini-implant placement, determining the ideal characteristics (shape, length, diameter and angulation). It also allows the precise and predictable mini-implant insertion.
Conclusion
The 3D technology represents the future of orthodontics, reducing the risks, chair-side time while providing the best treatment plan for the patient.
Acknowledgment
This research was conducted in the Orthodontic Research Center from Faculty of Dental Medicine, “Victor Babes” University of Medicine and Pharmacy, Timisoara.
References
- 1.Espeland L, Dowling P A, Mobarak K A, Stenvik A. (2008) Three-yearstability of open-bitecorrectionby 1-piece maxillaryosteotomy. , Am J Orthod DentofacialOrthop; 134, 60-66.
- 3.Ribeiro G L, Vieira G L, Ritter D, Tanaka O M, Weissheimer A. (2006) Non-surgicallyassisted rapid maxillaryexpansion in adults: A possible alternative. RevClínOrtod Dent Press. 5, 70-7.
- 4.Andrew J H. (1961) Rapid expansion of the maxillary dental arch and nasal cavity by opening the midpalatal suture. Angle Orthod. 31, 73-90.
- 5.Meikle M C. (2007) Remodeling the dento facialskeleton: the biological basis of orthodo nticsanddento facial orthopedics. J Dent Res. 86(1), 12-24.
- 6.Sun Z, Hueni S, Tee B C, Kim H. (2011) Mechanical strain at alveolar bone andcircummaxillarysuturesduring acute rapid palatal expansion. Am J Orthod Dentofacial Orthop. 139(3), 219-28.
- 7.Erverdi N, Okar I, Kucukkeles N, Arbak S. (1994) A comparison of twodifferent rapid palatal expansiontechniquesfromthepoint of rootresorption. , Am J Orthod Dentofacial Orthop 106(1), 47-51.
- 8.Baysal A, Uysal T, Veli I, Ozer T, Karadede I et al. (2013) Evaluation of alveolar bone lossfollowing rapid maxillary expansionusing cone-beam computedtomography. , Korean 43(2), 83-95.
- 9.Handelman C S, Wang L, BeGole E A, Haas A J. (2000) Nonsurgical rapid maxillaryexpansion in adults: report on 47 casesusingthe Haas expander. AngleOrthod. 70(2), 129-44.
- 10.Baccetti T, Franchi L, Cameron C G, McNamara JA Jr. (2001) Treatmenttiming for rapid maxillaryexpansion. AngleOrthod. 71(5), 343-50.
- 11.Gurel H G, Memili B, Erkan M, Sukurica Y. (2010) Long-termeffects of rapid maxillary expansion followed byfixed appliances. AngleOrthod. 80(1), 5-9.
- 12.Betts N J, Vanarsdall R L, Barber H D, Higgins-Barber K, Fonseca R J. (1995) Diagnosis and treatment of transversemaxillarydeficiency. , Int J Adult 10(2), 75-96.
- 13.Lee K J, Park Y C, Park J Y, Hwang W S. (2010) Miniscrew-assistednon surgical palatal expansion before ortho gnathics urgery for a patientwith severe mandibular prognathism. Am J Orthod Dento facial Orthop. 137(6), 830-9.
- 14.Christensen L. (2017) . Digital workflows in contemporary orthodontics. APOS Trends Orthod.;7: 12.
- 15.Hurt A J. (2012) . Digital technology in the orthodontic laboratory. Am J OrthodDentofacOrthop.;141: 245-247.
- 16.Joda T, Zarone F, Ferrari M. (2017) The complete digital workflow in fixed prosthodontics: a systematic review. BMC Oral Health.17:. 124.
- 17.Tarraf N E, Ali D M. (2018) Present and the future of digital orthodontics. , SeminOrthod 24, 376-385.
- 19.Graf S, Cornelis M A, HauberGameiro G, Cattaneo P M. (2017) Computer-aided design and manufacture of hyrax devices: can we really go digital?. , Am J OrthodDentofacOrthop 152(6), 870-874.
- 20.Harrell W E. (2009) 3D diagnosis and treatment planning in orthodontics. , SeminOrthod 15(1), 35-41.
- 21.Maino B G, Paoletto E, Lombardo L, Siciliani G. (2016) A three-dimensional digital insertion guide for palatal micro-implant placement. , J ClinOrthod L 12-22.
- 22.O De Gabriele, Dallatana G, Riva R, Vasudavan S, Wilmes B. (2017) The easy driver for placement of palatal micro-implants and a maxillary expander in a single appointment. , J ClinOrthod 51(11), 728-737.
- 23.Dietrich C A, Ender A. (2017) A validationstudy of reconstructed rapid proto typing models produced by two technologies. , AngleOrthod 87(5), 782-787.
- 24.Chakraborthy P, Krishnamurthy K. (2016) Digital Era of Orthodontics: A Review. , J DentOral Disord 2(1), 1-3.
- 25.D’haese J, Velde T Van De. (2012) Accuracy and Complications Using Computer-Designed Stereolithographic Surgical Guides for Oral Rehabilitation by Means of Dental Implants: A Review of the Literature. Clin Implant Dent Relat Res. 14(3), 321-335.
- 26.Zehnder M S, Connert T. (2016) Guided endodontics: accuracy of a novel method for guided access cavity preparation and root canal location. , IntEndod 49(10), 966-972.
- 27.Nojima L I, MDCG Nojima. (2018) Mini-implant selection protocol applied to MARPE. , Dental Press J Orthod 23(5), 93-101.
- 28.Popa A, Dehelean C, Calniceanu H, Watz C, Brad S et al. (2020) . A Custom-Made Orthodontic Mini-Implant—Effect of Insertion Angle and Cortical Bone Thickness on Stress Distribution with a Complex In Vitro and In Vivo Biosafety Profile.Materials,13, 4789.ISSN 1996-1944; CODEN: MATEG9 .
Cited by (1)
- 1.Harikrishnan Sruthi, Subramanian AravindKumar, 2023, 3D printing in orthodontics: A narrative review, Journal of International Oral Health, 15(1), 15, 10.4103/jioh.jioh_83_22