
Abstract
Plasma cell neoplasms of the thyroid gland are uncommon. They may occur either as a primary extraosseous (extramedullary) plasmacytoma or as secondary involvement by multiple myeloma (MM). Here, we report the case of a 62-year-old female, presenting with goiter and Hashimoto’s thyroiditis, in whom the histologic diagnosis of extraosseous plasmacytoma was unexpected. Histology of the total thyroidectomy specimen showed a diffuse infiltration of well-differentiated plasma cells against a background of Hashimoto’s thyroiditis. By immunohistochemistry, the majority of the plasma cells are positive for IgG heavy chain and kappa light chain (kappa:lambda ratio was about 6-7:1). PCR analysis of the immunoglobulin heavy and kappa chain (IGH, IGK) gene rearrangements showed clonal IGH and IGK gene rearrangements. MM was ruled out by lack of MM-related end organ damage and negative serum protein electrophoresis, immunofixation, and bone marrow biopsy. Although rare, plasmacytoma should be considered in patients presenting with enlarging thyroid gland and autoimmune thyroiditis. Histologic diagnosis and differential diagnoses are comprehensively discussed.
Author Contributions
Academic Editor: Rada M. Grubovic, Head of Department for Stem Cell Collection President of Macedonian Society for Transfusion Medicine, Macedonia.
Checked for plagiarism: Yes
Review by: Single-blind
Copyright © 2020 Matthew Crabtree, et al.
 This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Competing interests
The authors have declared that no competing interests exist.
Citation:
Introduction
Plasma cell neoplasm is characterized by clonal proliferation of plasma cells. Multiple myeloma (MM) is a type of plasma cell neoplasm characterized by bone marrow based proliferation of neoplastic plasma cells. It is often associated with an M protein in the patient’s serum and/or urine and evidence of MM-related end-organ damage: hypercalcemia, renal insufficiency, anemia, and/or bone lesions (CRAB). Sometimes the neoplastic plasma cells may form discrete/solitary mass without evidence of bone marrow involvement, known as plasmacytoma. Most localized plasmacytomas are found in the bone and are thus named solitary plasmacytoma of bone, while less than 5% of plasma cell neoplasms in one of the various extramedullary sites known as extraosseous (extramedullary) plasmacytoma 1. Extraosseous plasmacytoma can occur in any organ, but most frequently in the head and neck region, particularly in the upper airway and sinuses. Plasmacytoma involving thyroid gland is extremely rare, comprising only 1.4% of extraosseous plasmacytoma 2. True extraosseous plasmacytoma may be even rarer in the thyroid gland because some reported cases of thyroid plasmacytoma may actually represent thyroid involvement by MM 3. Here, we describe the case of a 62-year-old female, presenting with goiter and Hashimoto’s thyroiditis, in whom total thyroidectomy was performed and the subsequent histologic diagnosis of extraosseous plasmacytoma was a surprise.
Due to its rare occurrence, studies of extraosseous plasmacytoma of the thyroid were essentially all single case reports. Some of these cases were poorly documented. Therefore, up to date, the clinical pathological features are not fully understood. Continuous reporting of thyroid plasmacytoma will bring awareness of the disease, improve diagnostic accuracy, and provide better clinicopathologic correlation and perhaps better management of this tumor.
Case Report
A 62-year-old female smoker with past medical history of fibroids status post supracervical hysterectomy presented to Harbor-UCLA Medical Center with dysphagia and intermittent hoarseness. She noticed the enlargement of her neck about one and a half years prior to the presentation. On physical examination the thyroid was diffusely enlarged, more prominent on the left side, and firm, without tenderness. Ultrasound of the thyroid was done showing the enlarged, heterogeneous thyroid gland (right lobe: 4.3 x 6.7 x 2.3 cm; left lobe: 6.2 x 4.1 x7.1 cm) with several solid lesions, most compatible with a multinodular goiter. The fine needle aspiration of the right inferior thyroid nodule showed follicular cells with focal Hürthle change in a background of lymphocytes and scattered plasma cells, consistent with lymphocytic thyroiditis. Flow cytometric analysis was performed on the fine needle aspiration specimen and immunophenotypically aberrant T-cell or B-cell populations were not detected. The patient noticed a steady growth of her neck. Six months after her ultrasound examination, follow-up CT of her neck showed the thyroid gland was markedly enlarged ( right lobe: 7.0 x 8.8 x 4.7 cm; left lobe: 4.3 x 8.7 x 4.7 cm), multinodular and heterogeneous in appearance without evidence of discrete mass; the superior aspect of the right lobe of the thyroid gland wrapped posteriorly causing mild mass effect on the hypopharynx; the inferior aspect of the left lobe of the thyroid gland extended into the superior portion of the mediastinum and wrapped posteriorly displacing the trachea slightly rightward causing mild narrowing; no evidence of lymphadenopathy; no osseous lesions or acute fracture. The patient’s serum thyroid-stimulating hormone (TSH) was well-controlled (4.766 µIU/mL, reference range: 0.350-4.940 µIU/mL) by daily levothyroxine (LT4, 0.025 mg). She had high serum anti-thyroid peroxidase (TPO) antibodies (>600.0 IU/mL, reference range: ≤34.0 IU/mL), normal serum calcium (8.9 mg/dL, reference range: 8.9-10.3 mg/dL), and normal serum parathyroid hormone (PTH, 37 pg/mL, reference range: 15-65 pg/mL). Given the symptoms and the pressure effect, the patient underwent total thyroidectomy.
Gross examination of the thyroidectomy specimen showed a diffusely enlarged thyroid gland with bilateral bulging nodules weighing 276 grams, with right lobe measuring 8.8 cm in greatest dimension and left lobe measuring 8.7 cm in greatest dimension, firm in consistency, and having an intact capsule (Figure 1A). Sectioning at approximate 1 cm intervals showed the thyroid gland was near totally replaced by innumerable yellow tan solid nodules of variable sizes surrounded by fibrous bands (Figure 1B). There was no necrosis or calcification. No lymph nodes were found.
Figure 1.Gross examination of the thyroidectomy specimen shows a diffusely enlarged thyroid gland with bilateral bulging nodules (A, picture taken before fixation). A cut section shows the thyroid gland is replaced by innumerable yellow tan solid nodules of variable sizes surrounded by fibrous bands (B, picture taken after fixation).
Fifteen representative sections were submitted for microscopic examination and showed similar histologic features. The H&E stained sections of the thyroidectomy specimen revealed many nodules separated by fibrous bands (Figure 2A). There were a few scattered small foci of lymphocytic infiltrate with lymphoid follicle and germinal center formation, suggestive of Hashimoto’s thyroiditis (Figure 2B). The mantle zones were not expanded. The interfollicular areas were composed of some small lymphocytes and many plasma cells. Lymphoepithelial lesions, centrocyte-like cells, plasmacytoid lymphocytes, or large lymphoma cells were not present. The entire thyroid gland was extensively infiltrated by plasma cells. In some nodules remnant atrophic thyroid follicles were visible (Figure 2C), while in other nodules the thyroid parenchyma was almost entirely replaced by sheets of plasma cells (Figure 2D, 2E). The plasma cells were well–differentiated. They had an eccentrically-located nucleus, clock-face chromatin, inconspicuous nucleoli, and abundant cytoplasm (Figure 2F). There were no Dutcher bodies (intranuclear inclusions) or amyloid deposition. Hürthle cells were seen focally in one section. There was no evidence of papillary thyroid carcinoma in any sampled sections. Parathyroid tissue was identified in a few sections. Lymph nodes were not found.
Figure 2.Representative photomicrographs of the thyroidectomy specimen. Scanning power view shows many nodules separated by fibrous bands (A). There were a few scattered small foci of lymphocytic infiltrate with lymphoid follicle and germinal center formation, suggestive of Hashimoto’s thyroiditis (B). Low to medium power view showing a dense plasmacytic infiltrate with remnant atrophic thyroid follicles visible in some nodules (C), while in other nodules the thyroid parenchyma is almost entirely replaced by sheets of plasma cells (D, E). At high power, the plasma cells are well–differentiated; they have eccentrically-located nuclei, clock-face chromatin, inconspicuous nucleoli, and abundant cytoplasm (F). (H&E stain; original magnification, x 10 A, x 20 B, x 100 C and D, x 200 E, and x 400 F).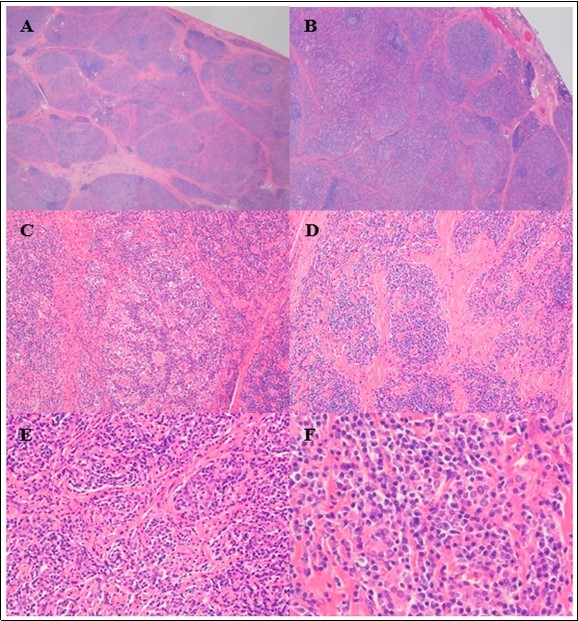
A panel of immunohistochemical (IHC) stains was performed including CD138 (Figure 3A), kappa (Figure 3B) and lambda (Figure 3C) light chains, immunoglobulin (Ig) A (Figure 3D), IgG (Figure 3E), IgM (Figure 3F), IgD (not shown), and IgG4 (not shown) heavy chains, CD3 (Figure 4A), CD20 (not shown), PAX-5 (Figure 4B), BCL6 (Figure 4C), BCL2 (Figure 4D), CD21 (Figure 4E), cyclin D1 (not shown), and ki67 (Figure 4F). The plasma cells were positive for CD138. The majority of the plasma cells were positive for IgG heavy chain and kappa light chain. Only small subsets of plasma cells were positive for IgA, IgM, or lambda light chain. The kappa to lambda ratio was about 6-7:1. Rare scattered plasma cells were positive for IgG4. CD3, CD20, and PAX-5 stains showed the lymphoid follicles were positive for CD20 and PAX-5 (B-cell markers), and the small lymphocytes surrounding the lymphoid follicles and the majority of the interfollicular small lymphocytes were T-cells (CD3 positive). The germinal centers were positive for BCL6 and negative for BCL2. CD21 stain highlighted undisrupted follicular dendritic cell meshworks. Ki67 stain showed appropriately high proliferation rates in germinal centers with polarization. There was no evidence of follicular colonization. Mantle zones (IgD and IgM positive) or marginal zones (IgD negative and IgM positive) were not expanded. Cyclin D1 was negative. Polymerase chain reaction (PCR) analysis of the immunoglobulin heavy and kappa chain (IGH, IGK) gene rearrangements was performed on one paraffin block of the thyroidectomy specimen at Quest Diagnostics by multiplex PCR followed by capillary electrophoresis and showed clonal IGH and IGK gene rearrangements, suggestive of the presence of clonal B-cells and/or plasma cells. Overall, the morphologic, immunohistochemical, and molecular features were consistent with extraosseous plasmacytoma in a background of Hashimoto’s thyroiditis.
Figure 3.A panel of immunohistochemical stains show the plasma cells are positive for CD138 (A). The majority of the plasma cells are positive for kappa light chain (B) and IgG heavy chain (E). Only small subsets of plasma cells are positive for lambda light chain (C), IgA (D), or IgM (F). (Immunoperoxidase staining; original magnification, x 100 A, x 200 B).
Figure 4.Immunohistochemical stains show the lymphocytes are predominantly T-cells (CD3 positive, A), with the lymphoid follicles highlighted by PAX-5 stain (B). The germinal centers are positive for BCL6 (C) and negative for BCL2 (D). CD21 stain highlights undisrupted follicular dendritic cell meshworks (E). Ki67 stain shows appropriately high proliferation rates in germinal centers with polarization. (Immunoperoxidase staining; original magnification, x 20 A and B, x 40 C).
Bone marrow aspirate and biopsy showed normocellular bone marrow with trilineage hematopoiesis and few polytypic plasma cells, with no lymphoid aggregates. No apparent monoclonal proteins were detected by serum protein electrophoresis (SPEP) and immunofixation (IFE). Urine protein electrophoresis (UPEP) was uninterpretable due to low total protein concentration. There was no evidence of MM-related end-organ damage (CRAB). Given the clinical presentation and the negative results of SPEP/UPEP and bone marrow examination, thyroid involvement by multiple myeloma was ruled out.
The patient recovered well from surgery and was put on 0.088 mg LT4 daily and 0.25 mcg calcitriol daily for iatrogenic hypothyroidism and hypoparathyroidism, respectively, and monitored with thyroid function tests. She was referred to radiotherapy services and did well for five months after surgery with no evidence of recurrence.
Discussion
We report the case of an extraosseous (extramedullary) plasmacytoma in the thyroid gland of an elderly woman who also had chronic lymphocytic thyroiditis (i.e. Hashimoto’s thyroiditis). Extraosseous plasmacytoma of the thyroid gland is a rare disease that can occur in patients with or without Hashimoto’s thyroiditis 2, 3, 4, 5, 6, 7. In fact, Hashimoto’s thyroiditis was detected in 63% of patients with extraosseous plasmacytoma of the thyroid gland 1. Hashimoto’s thyroiditis is an autoimmune disease affecting the thyroid gland and is the most common cause of hypothyroidism in developed countries 8. Women, typically 30-50 years old, are affected 10 times as often as men 8. Clinical findings include elevated TSH, low free thyroxine (fT4), and the presence of anti-TPO antibodies. Patients present with signs of hypothyroidism, such as fatigue, dry skin, constipation, and weight gain. Treatment consists of hormone replacement therapy. Histologicaly, Hashimoto’s thyroiditis is characterized by extensive lymphoplasmacytic infiltrate with germinal center formation and atrophic follicles with Hürthle cells. The lymphocytes are predominantly T cells. The plasma cells are polyclonal. Fibrosis may be increased. In a case of plasmacytoma arising in Hashimoto’s thyroiditis, the plasmacytoma components can be overlooked and misdiagnosed as Hashimoto’s thyroiditis, particularly at the early phase of the disease when the neoplastic plasma cell clone is small. Therefore, it is important to recognize the association between plasmacytoma and Hashimoto’s thyroiditis. IHC stains for kappa and lambda light chains should be performed to demonstrate clonality of the plasma cells when plasma cells are markedly increased in number, focally form sheets or nodules, or show atypical morphology such as enlarged cell sizes, enlarged nuclei, increased nuclear to cytoplasmic ratios, and prominent/distinct nucleoli.
A definitive diagnosis of plasmacytoma requires tissue biopsy. Diagnosis of plasmacytoma of the thyroid gland by fine needle aspiration (FNA) has been previously described 2, 3, though this is limited due to sampling bias and has the risk of misdiagnosis of a similar-appearing lesion such as medullary carcinoma of the thyroid 2 and small B-cell lymphoma with plasmacytic differentiation. While standard therapy for extraosseous plasmacytomas is radiotherapy and not surgery or chemotherapy, histological and immunohistochemical examination of surgical specimens is more reliable than cytological evaluation of FNA specimens 2, 9. In the present report, we described in detail the gross and microscopic findings of a plasmacytoma arising in Hashimoto’s thyroiditis.
Histologic diagnosis of plasmacytoma is usually straightforward. The neoplastic plasma cells may be scattered, in small clusters, in focal nodules, or in diffuse sheets. They vary from mature forms to immature, plasmablastic or anaplastic cells. Mature plasma cells are usually oval, with a round eccentric nucleus with a "spoke wheel" or “clock-face” chromatin without distinct or prominent nucleoli, commonly with abundant basophilic cytoplasm and a marked perinuclear hof. In immature forms, the cells typically have more dispersed nuclear chromatin, higher nuclear to cytoplasm ratios, and distinct/prominent nucleoli. Most plasmacytomas contain mainly mature plasma cells and are easily recognizable in tissue sections. Flow cytometry, immunohistochemistry, or in situ hybridization for immunoglobulin light chains can be useful in distinguishing a monotypic plasma cell neoplasm from polytypic reactive plasma cell infiltrates. In questionable cases, B-cell gene rearrangement studies can be performed to demonstrate the monoclonal nature. In rare poorly differentiated cases (e.g., plasmablastic or anaplastic plasmacytoma), CD38, CD138, MUM1 and EMA can be used to support plasma cell origin. Among these, CD138 is the most specific plasma cell marker.
Extramedullary involvement by MM has histologic and immunophenotypic features similar to those of extraosseous plasmacytoma; therefore it is necessary to rule out MM after a diagnosis of a plasmacytoma, including those of the thyroid gland. This requires a bone marrow biopsy, demonstration of the absence of lytic bone lesions, and no or minimal M spike 10.
Lymphomas with exuberant plasmacytic differentiation, especially lymphoplasmacytic lymphoma and marginal zone lymphoma, must be excluded before a diagnosis of plasmacytoma can be rendered. In fact, extranodal marginal zone lymphoma of mucosa-associated lymphoid tissue (MALT lymphoma) is relatively common in the thyroid, represents about 30% of thyroid lymphomas, and may be associated with Hashimoto’s thyroiditis 11. A search for areas of a biopsy with lymphocytic proliferation typical of these lymphomas should be performed. Flow cytometry is helpful in distinguishing lymphoma from plasmacytoma in that it can not only detect a monoclonal B-cell population which is diagnostic for B-cell lymphoma, but also demonstrate the immunophenotype of the plasma cells. Expression of CD19 and CD45 and lack of CD56 expression of the clonal plasma cells support lymphomas. By IHC, expression of CD20 and/or PAX-5 by lymphocytes in the lesion or by the plasmacytoid cells and expression of IgM rather than IgA or IgG heavy chain favor a diagnosis of lymphoma over plasmacytoma. In our case, the lymphocytes were predominantly T-cells, which is typically seen in reactive lymphocytic infiltrates rather than B-cell lymphomas. The germinal centers were positive for BCL6, negative for BCL2, and showed appropriately high proliferation rates with polarization by ki67 stain, consistent with reactive germinal centers. CD21 immunostain did not demonstrate a disrupted follicular dendritic cell meshwork pattern characteristic of follicular colonization in MALT lymphoma. Plasmacytoid lymphocytes were not seen, making lymphoplasmacytic lymphoma unlikely. Moreover, the plasma cells in our case express IgG, but not IgM, favoring plasmacytoma over lymphoma. Furthermore, flow cytometric analysis performed on the fine needle aspiration of the right inferior thyroid nodule did not detect light chain restricted B-cells, further against a diagnosis of B-cell lymphoma. It can be extremely difficult to differentiate plasma cell neoplasm from small B-cell lymphoma with prominent plasmacytic differentiation in small biopsies due to sampling of the areas with plasmacytic differentiation. However, our specimen was extensively sampled and no histologic or immunophenotypic features of B-cell lymphoma were noted.
The differential diagnoses of cases with anaplastic or plasmablastic plasmacytoma may include plasmablastic lymphoma. A history of immune deficiency and the presence of EBV by EBV-encoded small RNA (EBER) in situ hybridization are helpful in establishing the diagnosis of plasmablastic lymphoma. Only two cases of plasmablastic lymphoma were reported in the thyroid gland in the literature 12, 13. Both patients were immunocompetent. EBER was negative in both cases. It is debatable if these cases should be classified as plasmablastic lymphoma or anaplastic or plasmablastic plasmacytoma. According to the WHO 2017 classification, a descriptive diagnosis, such as “plasmablastic neoplasm, consistent with plasmablastic lymphoma or anaplastic plasmacytoma” is recommended 14. In our case, the plasma cells showed well-differentiated morphology, so plasmablastic lymphoma was not in the differential.
Medullary thyroid carcinoma (MTC) and malignant melanoma may sometimes superficially mimic plasmacytoma due to the plasmacytoid appearance of the tumor cells. Moreover, amyloid deposition can be seen in both MTC and plasma cell neoplasms. Fortunately, these tumors show immunophenotypes different from that of plasmacytoma and are thus readily excluded by IHC.
Hashimoto's thyroiditis was recently divided into IgG4‐plasma cell‐rich (IgG4 HT) and IgG4‐plasma cell‐poor (non-IgG4 HT) subtypes 15. Interestingly, Kojima and coauthors demonstrated intra-germinal center kappa light chain-restricted plasma cells in one IgG4 HT and one non-IgG4 HT cases, with no clonal rearrangement of the immunoglobulin heavy chain by PCR 16. Unfortunately, the number of these cases is too limited to clarify the clinicopathological significance. It is not clear whether these monotypic plasma cells were monoclonal in nature or whether these lesions may progress to plasmacytoma. A few cases of IgG4-producing MALT lymphoma 17, 18 and cases of IgG4 plasma cell myeloma 19, 20 have also been reported. The frequency of IgG4 myeloma seemed to correlate with the normal distribution of IgG4 isoform, with 6 out of 158 (4%) IgG myeloma cases expressed IgG4 19. Surprisingly, IgG4 extraosseous plasmacytoma has not been reported yet, possibly due to failure to apply IgG4 immunostain in plasmacytoma cases. Only rare scattered plasma cells in the present case were positive for IgG4.
In conclusion, we report one case of extraosseous plasmacytoma in the thyroid arising from Hashimoto’s thyroiditis. The findings indicate that plasmacytoma should be included in the differential diagnosis of thyroid goiter. Clinicians and pathologists need to be aware of the association of thyroid plasmacytoma and Hashimoto’s thyroiditis. In the present report, the histologic and immunophenotypic features of extraosseous plasmacytoma are described in detail, emphasizing differential diagnosis. The report adds another case to the limited literature currently available for extraosseous plasmacytoma of the thyroid gland.
Author Contributions Statement
PJ and XQ identified the case and conceived of the presented idea. MC and XQ performed the literature search and wrote the article. JCC prepared the figures/figure legends and helped shape the manuscript. XQ supervised.
References
- 1.Meccawy A A. (2010) Plasmacytoma of the thyroid gland: case report and review of the literature. JKAU: Med Sci. A.D. /1431 A.H.) doi: 10.4197/Med. 17-2.7 17(2), 83-92.
- 2.Bhat V, Shariff S, Reddy R A. (2014) Extramedullary plasmacytoma of thyroid - a mimicker of medullary carcinoma at fine needle aspiration cytology: a case report. , J Cytol 31(1), 53-56.
- 3.Ridal M, Ouattassi N, Harmouch T, Amarti A, Alami M N. (2012) Solitary extramedullary plasmacytoma of the thyroid gland. Case Rep Otolaryngol.
- 4.Refai F, Gomaa W, Abdullah L. (2019) A case report of thyroid plasmacytoma and literature update.J MicroscUltrastruct. 8(2), 75-79.
- 5.Beguin Y, Boniver J, Bury J, Defraigne J O, Detroz B. (1987) Plasmacytoma of the thyroid: a case report, a study with use of the immunoperoxidase technique, and a review of the literature. , Surgery 101(4), 496-500.
- 6.Kovacs C S, Mant M J, Nguyen G K, Ginsberg J. (1994) Plasma cell lesions of the thyroid: report of a case of solitary plasmacytoma and a review of the literature. , Thyroid 4(1), 65-71.
- 7.Puliga G, Olla L, Bellisano G, N Di, Ganau M. (2011) Solitary extramedullary plasmacytoma of the thyroid gland associated with multinodular goiter: case report and review of the literature. , Pathologica 103(3), 61-63.
- 8.Mincer D L, Jialal I. (2020) Hashimoto thyroiditis. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing. Available from: https://www.ncbi.nlm.nih.gov/books/NBK459262/.
- 9.Tsang R W, Campbell B A, Goda J S, Kelsey C R, Kirova Y M. (2018) Radiation therapy for solitary plasmacytoma and multiple myeloma: guidelines from the international lymphoma radiation oncology group. , Int J Radiat Oncol Biol Phys 101(4), 794-808.
- 10.Sahu K K, Singh P, Malhotra P, Srinivasan R. (2019) Thyroid plasmacytoma: a rare cause of hoarseness of voice. , Indian J Nucl Med 34(1), 78-80.
- 11.Shrestha P, Aderhold K, Swierczynski S, Lin C, Herb R. (2018) Primary thyroid MALToma– a rare diagnosis of an unassuming thyroid nodule. , J Community Hosp Intern Med Perspect 8(1), 42-45.
- 12.Ahmed F, Mundada M C, Murthy S S, Rajappa S J. (2015) Plasmablastic lymphoma developing in thyroid: a rare entity in an immunocompetent individual. Egypt J Haematol. Available from: http://www.ehj.eg.net/text.asp?2015/40/3/150/164743. 40, 150-152.
- 13.Gallagher T M, Narayana S, Malysz J. (2018) Primary plasmablastic thyroid lymphoma: a case report. , AACE Clinical Case Reports 4(3), 191-194.
- 14.Campo E, Stein H, Harris N L.(2017).Plasmablastic lymphoma.In Swerdlow SH,CampoE,Harris NL,Jaffe ES,Pileri SA,Stein H, Thiele J. (Eds):WHO classification of tumours of haematopoietic and lymphoid tissues (revised 4thedition).IARC:Lyon. 321-322.
- 15.Li Y, Bai Y, Liu Z, Ozaki T, Taniguchi E. (2009) . Immunohistochemistry of IgG4 can help subclassify Hashimoto’s autoimmune thyroiditis. Pathol Int 59, 636-641.
- 16.Kojima M, Hirokawa M, Kuma H, Nishihara E, Masawa N. (2010) Distribution of IgG4- and/or IgG-positive plasma cells in Hashimoto’s thyroiditis: an immunohistochemical study. , Pathobiology 77, 267-272.
- 17.Sato Y, Ohshima K, Ichimura K, Sato M, Yamadori I. (2008) Ocular adnexal IgG4-related disease has uniform clinicopathology. , Pathol Int 58, 465-470.
- 18.Tan C L, Ong Y K, Tan S Y, Ng S B. (2016) IgG4-positive extranodal marginal zone lymphoma arising in Hashimoto's thyroiditis: clinicopathological and cytogenetic features of a hitherto undescribed condition. , Histopathology 68(6), 931-937.
Cited by (1)
- 1.Pasricha Sunil, Diwan Himanshi, Bansal Divya, Jajodia Ankush, Agarwal Mudit, et al, 2022, Intrathyroidal Plasmacytoma with Pleomorphic Multilobated Bizarre Cells: A Rare Primary Clinicopathological Presentation Mimicking Anaplastic Carcinoma of Thyroid, Head and Neck Pathology, 16(4), 1257, 10.1007/s12105-022-01465-2