
Abstract
Introduction:
The Roux-en-Y Gastric Bypass (RYGB) has been one of the most popular surgeries in the USA for years. While many models have been made to investigate the factors that affect weight loss, these factors are still highly debated.
Objective:
To create a model that predict performance of RYGB patients.
Methods:
110 out of 344 patients who received a RYGB at a single institution between Jan 2010 and April 2014 were included in this study. Data was collected retrospectively. Patients were included if they had greater than 1 year follow up with at least three follow up points and could be modeled with r2>0.95. All patients were one year beyond surgery, while 40 were completely lost to follow up, 104 at 1 month, 138 at 3 months, 188 at 6 months, and 225 at one year. 9 patients were not included because they did not meet the criteria of the study. Patients were divided into quartiles based on percentage excess weight loss (%EWL) at one year. Multivariate analysis was performed to determine the significant factors that influence patients being in the first quartile of weight loss (17-60% %EWL).
Results:
Only males with a Body Mass Index (BMI) above 44 and females with a BMI above 64 were found to be predictive of patients being in the first quartile. Our model has Positive and Negative predictor values of 66% and 80% respectively with sensitivity and specificity of 29% and 95% respectively.
Conclusions:
An model to predict %EWL was created, only gender and pre-operative BMI were found to be significant factors. In general females have better outcomes with higher BMI’s than do males. This information should be discussed with patients when deciding a procedure. However, more studies are needed for validation of these results.
Author Contributions
Academic Editor: Amit Surve, Bariatric Research Specialist at Bariatric Medicine Institute, Utah, U.S.A.
Checked for plagiarism: Yes
Review by: Single-blind
Copyright © 2016 Daniel cottam, et al.
 This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Competing interests
The authors have declared that no competing interests exist.
Citation:
Introduction:
The Roux-en-Y Gastric Bypass (RYGB) has been the most popular surgery for weight loss in the USA for many years 1.Surgeons have tried to develop many models to predict the factors that result in weight loss success. Many models look into predicting complications or mortality and are not so much concerned with weight loss results 2, 3, 4, 5, 6.
Some models out there do predict weight loss. The first one in this category was from Mor et al who showed that weight loss results of RYGB are determined from early post-operative visits 7. They found that gender, pre-operative BMI, and weight loss at 1-month post-operative determine weight loss results. Their model showed strong predictive power, however, there was no way to apply it to an individual surgeons practice. However, this was a good start for making models of weight loss.
Other studies looked more into the psychological reasons for weight loss failure. These studies focused on looking at support systems in place with patients and strict psychological tests to determine how well patients will do post-operatively 8, 9. These studies while accurate are hard to reproduce since they do publish an exact model to follow. Our group wanted to be able to use a model to predict patient outcomes and without publishing an exact model we could not apply it to our practice. Our group desired to have an easy to use model that used data normally gathered in office without changing program protocol.
In 2015 Wise et al used a newer innovation in artificial neural networks to make a workable pre-operative prediction of weight loss model 10. Their results were remarkable with their accuracy and prediction power. Most importantly their model is simple to use. This model taught us that the most important thing to look for models that predict weight loss outcomes is ease of use. Otherwise it will not be used. Our studies goal is to add to the current literature with a user friendly model for surgeons to manage post-operative outcomes of their patients.
Methods:
344 patients underwent primary RYGB surgery at a single private practice institution between Jan 2010 and April 2014. Demographic data and comorbid conditions were collected. All revisional patients were excluded from this study. Patients with a BMI over 65 were excluded from the study. Data was gathered retrospectively on a prospectively kept database. Patients were diagnosed with type 2 diabetes, hypertension, or gastroesophageal reflux disease (GERD) if they were on medications for these diseases. Sleep apnea was only counted if the patient had the diagnosis from a sleep study. Severity of these diseases was not assessed.
To be included for evaluation patients had to have follow up greater than one year with at least three follow up points in the first year. This data allowed weight loss to be interpolated at specific time points through non-linear regression. All patients needed an r² value of at least .95. (Simply, this means that at most 5% of the weight loss cannot be explained by simply time since the operation, but by extraneous variables).
Out of the 344 patients only 110 met the criteria for this study. Out of the 244 40 were completely lost to follow up, 104 at 1 month, 138 at 3 months, 188 at 6 months, 225 at 1 year. The 9 additional patients did not meet the other criteria of this study. Comparisons between the whole population and study population were performed for age, sex, weight, height, and body mass index (BMI). Comparisons are found on Table 1. There were no statistically significant differences in these groups.
Table 1. A demographic comparison between the study patients to general patient population| Study Patients | All Patients | P Value | |
| N | 110 | 344 | |
| BMI (kg/m2) | 49.4±11.7 | 47.4±7.9 | .345 |
| Weight | 302.8±83.4 | 293.1 ±63.2 | .415 |
| Height (inches) | 65.4±4.03 | 65.6±3.8 | .601 |
| Age | 44.1±12.5 | 45.2±12.9 | .9 |
| Male/Female | 13/97 | 68/276 | .08 |
From each patient’s weight at one year, percentage excess weight loss (%EWL) was calculated as the percentage of weight lost above the weight the patient would be if their BMI was 25. Patients were then divided into quartiles based on %EWL at one year.
Multiple logistic regression was run using each individual patient’s data to determine the significant variables that effect weight loss. Variables studied were gender, age, BMI, sleep apnea, diabetes, GERD, and hypertension. The Wald statistic was used in order to determine significance of each variable. A model was then made using multiple logistic regression with only the variables that significantly affect weight loss. The efficacy of the model was determined using a chi-squared test, likelihood ratio, area under the receiver operator characteristic (ROC) curve and the Hosmer-Lemeshow Statistic. The cut off value of the regression was optimized using a ROC curve. This was found using an index takes into account probability of patients ending up in the bottom quartile. All statistical analysis was done using SigmaPlot statistical software.
Results:
110 patients met the inclusion criteria. Of these patients 97 were female (86%). The preoperative demographics are shown in Table 2. The average %EWL at one year was 75% ± 23%. %EWL quartiles are quartile 1 17-60%, quartile 2 60-74%, quartile 3 74-88%, quartile 4 >88%. Preoperative BMI and Gender were found to be significant factors of RYGB patients being in the bottom quartile by multiple logistic regression analysis. Females were found to lose more excess weight by our model. The higher the patient’s BMI the more likely they were to not lose adequate %EWL by the model. Diabetes, hyperlipidemia, sleep apnea, GERD, hypertension, and age were not found to be significant factors in predicting weight loss outcomes at one year (Table 3).
Table 2. Pre-Operative Demographic characteristics for RYGB patients| Overall | Quartile 1 | Quartile 2 | Quartile 3 | Quartile 4 | P value | |
| N | 110 | 28 | 27 | 28 | 27 | |
| BMI | 46.7±7.9 | 51±8.1 | 49.7±7.3 | 45±7.3 | 40.9±4.6 | <.001 |
| Weight | 284.8±56.6 | 314.9±57.6 | 296.4±50.4 | 271.5±54.3 | 255.8±46.8 | <.001 |
| Height | 65.3±3.9 | 65.6±5.2 | 64.7±3.4 | 65±3.4 | 66.1±3.5 | .329 |
| Age | 45.1±12.9 | 46.6±11.5 | 42.8±13.4 | 45.2±13 | 45.6±14.1 | .824 |
| Male/Female | 13/97 | 8/20 | 0/27 | 3/25 | 2/25 | .008 |
| Excess Weight Loss | 75%±23% | 47%±12% | 67%±4% | 82%±5% | 104%±13% | <.001 |
| Range | 17%-134% | 17%-60% | 62%-73% | 74%-88% | 90%-134% | |
| Diabetes | 31 (28%) | 11 (39%) | 6 (22%) | 7 (25%) | 7 (26%) | .496 |
| Sleep Apnea | 43 (39%) | 17 (61%) | 8 (30%) | 11 (39%) | 7 (26%) | .037 |
| GERD | 42 (38%) | 10 (36%) | 11 (41%) | 11 (39%) | 10 (37%) | .994 |
| Hyperlipidemia | 33 (30%) | 4 (14%) | 11 (41%) | 10 (36%) | 8 (30%) | .201 |
| Hypertension | 52 (47%) | 17 (61%) | 11 (41%) | 14 (50%) | 10 (37%) | .237 |
| Variables | P value |
|---|---|
| Age | .646 |
| Gender | .006 |
| BMI | .002 |
| Diabetes | .298 |
| Sleep apnea | .622 |
| GERD | .638 |
| Hypertension | .154 |
| Hyperlipidemia | .23 |
A model was obtained by running multiple logistic regression where success is being in the bottom quartile. The predictive model obtained by multiple logistical regression is if males are above a BMI of 63.7 and females are above a BMI of 44.1 they will not be able achieve an %EWL of 60% at 1 year. This model has a Positive and Negative predictor value of 66% and 80% respectively with a sensitivity and specificity of 29% and 95% respectively. Our model also has an area under the curve of .75 (Figure 1).
Figure 1.ROC curve analysis. This is measured in terms of sensitivity and specificity. Anything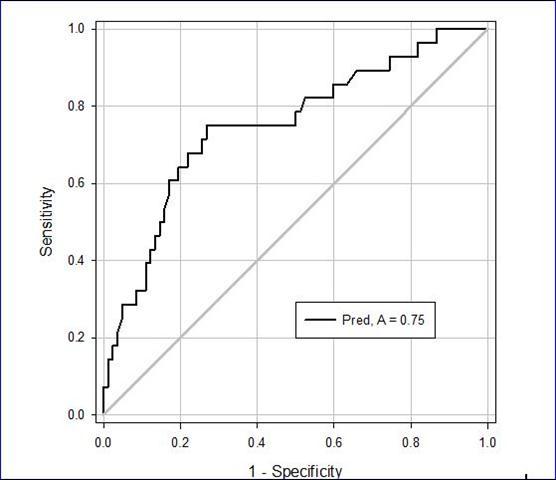
Discussion:
The purpose of this study was to use simple data collection points in order to come up with a mathematical model to predict RYGB outcomes. This equation presented in the discussion sections is easy to perform and requires no advance math skills and can be done on any simple calculator. Many varying models have been made to predict weight loss after surgery but they are complex and burdensome and our paper is unique because we have actually shown the reader the equation validating our thesis. We believe that as others apply the same methods to their own data sets that the model will become both more predictive and better refined. With a variety of procedures it is certain that there is not a procedure that fits for all. In order to help patients, most surgeons match objectives with likely outcomes. Most quote average %EWL, but this is vastly inaccurate. In order to be more accurate than average %EWL, we used multi-variate analysis.
Our cohort had an average of 75% %EWL at one year. This is well within the range of published %EWL values at one year 11, 12, 13, 14, 15. This adds significance to our study as our population is similar to most populations throughout the USA.
One interesting thing about our model is that it can indirectly show that within limits that technical variances and pre-operative patient behavior are not responsible for one year outcomes. Our model predicts accurately without having any of these factors. With this information more studies into predictive modeling should be made.
Most investigators have defined success of a bariatric surgery as greater than 50% %EWL 9. We fully agree with this definition and powered our analysis to predict the bottom quartile of patients and our bottom quartile was defined as less than 60% EWL. However, we postulate, with standard weight regain seen in years three through five with the RYGB it can be assumed that all the patients in our bottom quartile will fail by this definition. There are many more factors than simple %EWL to define what success and failure is but this is a comparative model and will allow others who follow to refine and compare to. It also gives surgeons an easy way to manage expectations.
Many factors have been found to influence the outcome of the RYGB. These include race, initial BMI, hypertension, gender, height, age, diabetes, ghrelin, and initial weight 16, 17, 18, 19, 20, 21. All have been found to be significant factors in different studies. However, many of these have only been found to be significant in one study and other studies have found it to be insignificant. Some factors have only been studied once, and have been found to significantly affect weight loss. These include caloric intake capacity, water/soda intake, MMPI-2-RF findings, eating disorders, and breast cancer biomarker 8, 22, 23, 24, 25. These factors are not usually collected and each only have one study that investigate them, so we did not include them in this study.
In light of these considerations we sought to make an easily used predictive model by only including things that should already be collected in any practice.
Our finding of only BMI and gender effecting weight loss is consistent in the literature and correlates with our previous work. In 2009 we also found that the only significant effectors of weight loss at one year were gender and BMI 26. This study correlates directly with our results that other factors are not significant in predicting excess weight loss at one year.
However, we are not completely sure to as gender was found to be a significant factor. We can only postulate on the reasons. It may have to do with the fact that females tend to come in for follow ups on a more regular basis. With BMI the reasons are clearer. The postulated reason we have come up with is that the RYGB may not incorporate enough malabsorption to significantly help those who are super obese.
Our model shows that diabetes is not a significant factor in weight loss at 1 year. The literature has been unclear on this issue and we hope our study ultimately helps determine whether or not if affects weight loss after RYGB. 10, 27
We also did not find GERD to be a factor which agrees with previously published literature for the RYGB 28. Sleep apnea has not previously been shown to effect weight loss in studies which agrees with our results as sleep apnea was not found to be a significant factor. However sleep apnea has been linked to various complications and mortality 29. For this reason, we chose to look at sleep apnea as it has some effect on patient outcomes if not weight outcomes.
Hyperlipidemia was also not found to be a significant factor in weight loss at one year. Hyperlipidemia has not previously been shown to effect weight loss which agrees with our findings.
Literature is split on whether hypertension effects weight loss however in our study we found that it had no effect on eventual weight loss 10, 29, 30. Literature is also split of whether age effects weight loss however we did not find it to be significant 7, 23.
Some may criticize our total follow up population of 110 patients out of 344. However, this does not affect our ability to examine the effects of different comorbidities on weight loss and their interaction as we are looking at weight loss as the output and 110 patients is easily enough statistically to draw weight loss conclusions from the variables presented. This is reflected in the high p-values of the comorbidities analysis. Additionally, this is especially important if you believe that those who don’t follow up have worse outcomes than those that do. In the first study of its kind Hunter Mehaffey J et al demonstrated that those that are lost to follow up do not have any statistical difference in outcomes to those who regularly follow up 31. We have shown that there are subclasses of RYGB who have high failure rates that affect them in spite of what many would classify as good follow up.
Only having 13 male patients in this study was a severe limitation. We included it in the analysis since it was pertinent and gave us high p values and we could not think of a reason to exclude them. Yet, we acknowledge the limited data set.
It is important to note that this model predicts only one female ending up in the bottom quartile of the 97 females in the study. It is not until the female patients exceed a BMI of 64 can we positively predict if they will be in the bottom quartile. While in the males, this happens at a relatively low BMI of 44. In our study 8 of the 13 males who were eligible ended up in the bottom quartile. This could represent selection bias towards males who failed followed up in our practice while those who succeeded did not. Ideally we would like to see a larger sample size to validate both our 2009 paper 26 and this one as well.
The last important limitation of the paper is its low sensitivity. This is not surprising as our numbers were low and we hope as we acquire larger data sets we can raise this number but in order to not alarm patients whom we discuss our results with we elected to model our patients for the highest specificity possible and accept the low sensitivity as part of the model.
Conclusion:
We have developed a model that can be used to help predict weight loss results after the RYGB. Only gender and pre-operative BMI were found to be significant factors. In general females have better outcomes with higher BMI’s than do males. This model can be used preoperatively to allow surgeons to educate patients about weight loss goals and design better post-operative treatments pre-operatively. This information should be discussed with patients when deciding a procedure.
References
- 1.Esteban Varela J, Nguyen N T.(Feb2015,12) Laparoscopic sleeve gastrectomy leads the U.S. utilization of bariatric surgery at academic medical centers. Surg Obes Relat Dis.
- 2.Lee W J, Hur K Y, Lakadawala M. (2013) Predicting success of metabolic surgery: age, body mass index, C-peptide, and duration score. Surg Obes Relat Dis. 9, 379-84.
- 3.Ramanan B, Gupta P K, Gupta H, Fang X, Forse R A. (2012) Development and validation of a bariatric surgery mortality risk calculator. , J Am Coll Surg; 214, 892-900.
- 4.Lorente L, Ramón J M, Vidal P. (2014) Obesity surgery mortality risk score for the prediction of complications after laparoscopic bariatric surgery. Cir Esp. 92, 316-23.
- 5.Adamina M, Steffen T, Tarantino I, Beutner U, Schmied B M et al. (2015) Meta-analysis of the predictive value of C-reactive protein for infectious complications in abdominal surgery. , Br J Surg; 102, 590-8.
- 6.Fernandez AZ Jr, Demaria E J, Tichansky D S. (2004) Multivariate analysis of risk factors for death following gastric bypass for treatment of morbid obesity. , Ann Surg; 239, 698-703.
- 7.Mor A, Sharp L, Portenier D, Sudan R, Torquati A. (2012) Weight loss at first postoperative visit predicts long-term outcome of Roux-en-Y gastric bypass using Duke weight loss surgery chart. Surg Obes Relat Dis. 8, 556-60.
- 8.Marek R J, Tarescavage A M, Ben-Porath Y S, Ashton K, Merrell Rish J et al.(Apr2015,2) Using presurgical psychological testing to predict 1-year appointment adherence and weight loss in bariatric surgery patients: predictive validity and methodological considerations. Surg Obes Relat Dis.[Epub ahead of print].
- 9.Livhits M, Mercado C, Yermilov I. (2010) Behavioral factors associated with successful weight loss after gastric bypass. Am Surg. 76, 1139-42.
- 10.Wise E S, Hocking K M, Kavic S M.(May2015,28) Prediction of excess weight loss after laparoscopic Roux-en-Y gastric bypass: data from an artificial neural network. Surg Endosc. [Epub ahead of print].
- 11.Velcu L M, Adolphine R, Mourelo R, Cottam D R, Angus L D. (2005) Weight loss, quality of life and employment status after Roux-en-Y gastric bypass: 5-year analysis. Surg Obes Relat Dis. 1, 413-6.
- 12.Nguyen N T, Slone J A, Nguyen X M, Hartman J S, Hoyt D B. (2009) A prospective randomized trial of laparoscopic gastric bypass versus laparoscopic adjustable gastric banding for the treatment of morbid obesity: outcomes, quality of life, and costs. , Ann Surg; 250, 631-41.
- 13.Kalfarentzos F, Skroubis G, Kehagias I, Mead N, Vagenas K. (2006) A prospective comparison of vertical banded gastroplasty and Roux-en-Y gastric bypass in a non-superobese population. Obes Surg. 16, 151-8.
- 14.Park J Y, Kim Y J. (2015) Laparoscopic sleeve gastrectomy in obese Korean patients: up to 4-year follow-up in a single center. Ann Surg Treat Res. 88, 246-52.
- 15.Costa R C, Yamaguchi N, Santo M A, Riccioppo D, Pinto-Junior P E. (2014) Outcomes on quality of life, weight loss, and comorbidities after Roux-en-Y gastric bypass. Arq Gastroenterol. 51, 165-70.
- 16.Sczepaniak J P, Owens M L, Garner W, Dako F, Masukawa K et al. (2012) A simpler method for predicting weight loss in the first year after Roux-en-Y gastric bypass. , J Obes;2012: 195251.
- 17.Chen E Y, McCloskey M S, Doyle P.Body mass index as a predictor of 1-year outcome in gastric bypass surgery. , Obes Surg.2009 19, 1240-2.
- 18.Ma Y, Pagoto S L, Olendzki B C. (2006) Predictors of weight status following laparoscopic gastric bypass. Obes Surg. 16, 1227-31.
- 19.Manning S, Pucci A, Carter N C. (2015) Early postoperative weight loss predicts maximal weight loss after sleeve gastrectomy and Roux-en-Y gastric bypass. Surg Endosc. 29, 1484-91.
- 20.Couce M E, Cottam D, Esplen J, Schauer P, Burguera B. (2006) Is ghrelin the culprit for weight loss after gastric bypass surgery? A negative answer. Obes Surg. 16, 870-8.
- 21.Vendrell J, Broch M, Vilarrasa N. (2004) Resistin, adiponectin, ghrelin, leptin, and proinflammatory cytokines: relationships in obesity. Obes Res. 12, 962-71.
- 22.Sauter E R, Mitchell J E, Kliethermes B, Crosby R D.Breast cancer biomarkers predict weight loss after gastric bypass surgery. , BMC Res Notes.2012.31;5: 82.
- 23.Alfonsson S, Sundbom M, Ghaderi A. (2014) Is age a better predictor of weight loss one year after gastric bypass than symptoms of disordered eating, depression, adult ADHD and alcohol consumption? Eat Behav. 15, 644-7.
- 24.Gras-Miralles B, Haya J R, Moros J M. (2014) Caloric intake capacity as measured by a standard nutrient drink test helps to predict weight loss after bariatric surgery. Obes Surg.24:. 2138-44.
- 25.Coleman K J, Brookey J. (2014) Gender and racial/ethnic background predict weight loss after Roux-en-Y gastric bypass independent of health and lifestyle behaviors. Obes Surg. 24, 1729-36.
- 26.Cottam D R, Fisher B, Sridhar V, Atkinson J, Dallal R. (2009) The effect of stoma size on weight loss after laparoscopic gastric bypass surgery: results of a blinded randomized controlled trial. Obes Surg. 19, 13-7.
- 27.Schauer P R, Burguera B, Ikramuddin S. (2003) Effect of laparoscopic Roux-en Y gastric bypass on type 2 diabetes mellitus. , Ann Surg; 238, 467-85.
- 28.DuPree C E, Blair K, Steele S R, Martin M J. (2014) Laparoscopic sleeve gastrectomy in patients with preexisting gastroesophageal reflux disease : a national analysis. , JAMA Surg; 149, 328-34.
- 29.Perugini R A, Mason R, Czerniach D R. (2003) Predictors of complication and suboptimal weight loss after laparoscopic Roux-en-Y gastric bypass: a series of 188 patients. , Arch Surg; 138, 541-6.