
Author Contributions
Academic Editor: Asaad Ghane, Mansoura ophthalmic center, mansoura university, mansouraam
Checked for plagiarism: Yes
Review by: Single-blind
Copyright © 2023 ORAIN Edward Paul, et al.
 This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Competing interests
The authors have declared that no competing interests exist.
Citation:
Introduction
Adenoid cystic carcinoma (ACC) of the lacrimal gland is a rare tumor, representing 1.6% of all orbital tumors but is the most frequent malignancy seen of lacrimal gland epithelial tumor type. 1 It typically affects young adults with a peak incidence in the fourth decade and a slight preference or women. 2 Clinical manifestations of this malignancy include proptosis, pain, dystopia, eyelid fullness or swelling, diplopia and motility deficits. On MRI and CT scan, ACC often reveals a solid tumor in the superotemporal orbit, causing proptosis with bone erosion and possible calcification. 3
ACC has a relatively rapid progression of fewer than 6 months compared to benign neoplasms of the lacrimal gland, which shows signs and symptoms for more than a year. 4
Treatment for ACC of the lacrimal gland remains controversial. Some authors advocated conservative like plaque radiotherapy vs. radical surgical therapy followed by radiotherapy and or chemotherapy. 2 Despite these modalities, this malignant tumor has a poor overall prognosis that tends to recur and metastasize. We report a case of ACC seen in a 36-year-old male, its clinical course, radiographic presentation, treatment challenge and outcome.
Case Description
This is a case of a 36-year-old male who presented with a 3-month history of inferior displacement of his left eye (Figure 1). Associated clinical signs and symptoms include fullness over the left upper eyelid, periorbital pain and proptosis. On systemic review, he had weight loss and the presence of left anterior cervical lymphadenopathies were not noted. Ophthalmologic examination revealed visual acuity of 6/6 in both eyes, 2-3 mm briskly reactive to light pupils, and unremarkable anterior & posterior segment findings. Examination of the orbit showed fullness over the left upper eyelid with no palpable mass, inferior or downward displacement of the left eye and non-axial proptosis, and limitation (-3) of the left eye on upward gaze.
Figure 1.Periorbital inspection showing fullness of the left upper eyelid with inferomedial displacement of the left eye
Orbital MRI showed a 2.6 x 2.9 x 3.2 cm (cc x w x ap) heterogeneously enhancing mass seen in the extraconal space (superolateral aspect) likely arising from the left lacrimal gland (Figure 2). The lesion exhibits mixed (predominantly hyperintense T2 wave and predominantly intermediate T1W) signals. Mass effect was noted compressing the retrobulbar fat with resultant medial displacement of the optic nerve, inferior displacement and anterior protrusion of the globe. The mass abuts the superior rectus, levator palpebrae superioris and lateral rectus muscle.
Figure 2.Orbital MRI showing an enhancing lacrimal gland mass (Axial & Coronal Views), left
The patient was surgically managed with lateral orbitotomy and removal of the orbital mass under general anesthesia last July 23, 2019 (Figure 3). Skin marking was drawn over the following orbital landmarks: superior, inferior, lateral orbital rim and zygoma. A Stallard-Wright S-shaped lateral orbitotomy incision was made and dissection was carried down to the orbital rim periosteum. After incision of the periosteum, the lateral orbital rim was exposed and markings were placed for the periosteal flaps. Osteotomy was done using a bone chisel and mallet). After bone removal, part of the mass was visible, firm and fixed to surrounding structures. After careful dissection and release, the lesion was excised. No gross bone deformities were noted. The lateral orbital rim was repositioned . The periosteum was then closed over the bone to secure its position. The drain was placed, followed by subcutaneous closure then skin closure.
Figure 3.Skin marking of landmarks and incision B. Lateral orbital rim exposed and markings placed C. Osteotomy D. After bone removal, part of the mass is seen E. Lateral orbital rim was repositioned F. Day 11 post-op, grossly there’s marked improvement of previous globe displacement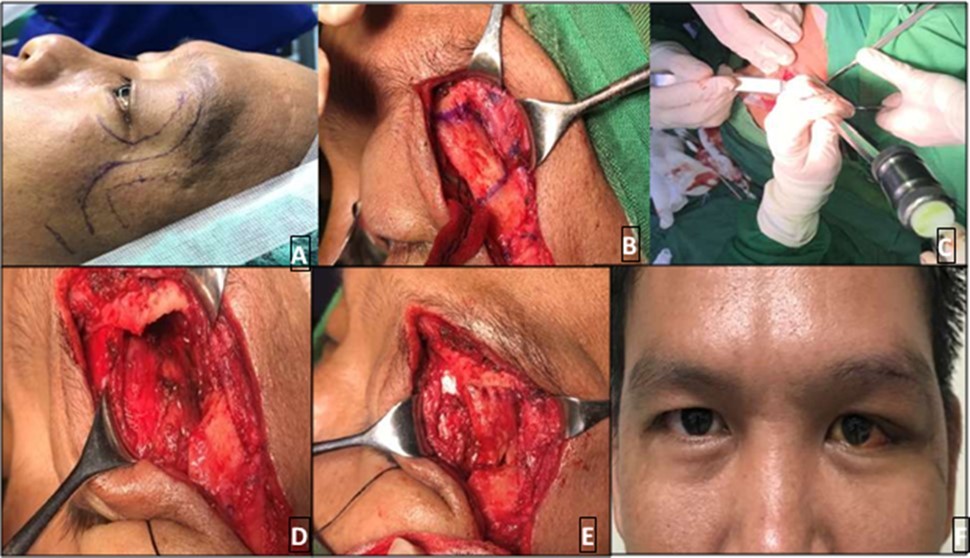
Histopathologic study described that the mass consisted of a piece of dark brown ovoid soft tissue measuring 3.5 x 3.2 x 1.5 cm .The external surface is rough with a mucosal defect measuring 0.8cm at its widest diameter. Cut sections show light brown, variegated solid surface. Microsections disclose sheets and nests of neoplastic cells forming solid and cribriform patterns .The histologic report showed adenoid cystic carcinoma with lymphovascular and perineural invasion. The surgical margins are positive for tumor involvement.
He was referred to Oncology Service for further evaluation and planned radiotherapy to address possible tumor residual and prevent local recurrence. While surgical removal has improved globe position and reduced proptosis of patient’s left eye (Figure 3), treatment was not completed. Prognosis and the need for close follow-up were discussed extensively with the patient; however, he moved to another area and was lost to follow up.
The patient followed two years afterwards due to palpable mass noted on the same site . He was seen by the service again and was referred to Oncology Department. On repeat imaging, there was tumor recurrence with intracranial extension . Systemic work-up revealed pulmonary metastasis. Prognosis was discussed and while exenteration was advised, he was need keen for this and opted for a globe-sparing procedure. A repeat lateral orbitotomy with debulking of the tumor was done. He continues to undergo chemotherapy (on 5th cycle) and follow up . Figure 4, Figure 5
Figure 4.Orbital Mass, left 4B. Cribriform or Swiss-Cheese Pattern 4C. Lymphovascular and perineural invasion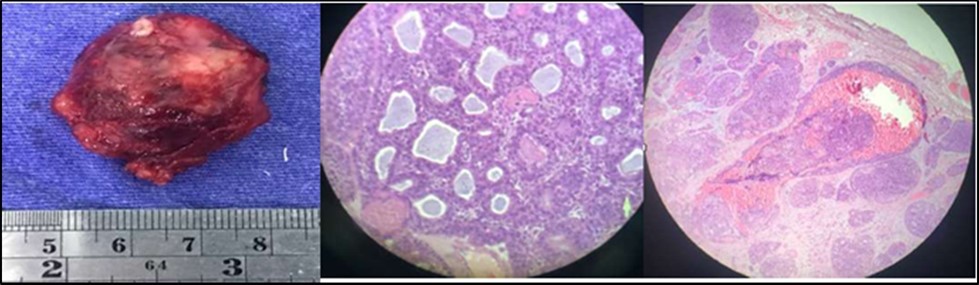
Figure 5A.Patient seen two years after the first orbitotomy and tumor excision, with recurrence of mass in the superotemporal orbit and globe displacement. B. Orbital CT scan (axial and coronal sections) revealed a 2.2 x 2.4 x 3.3 cm lobulated, heterogeneously enhancing soft tissue mass seen centered in the left lacrimal gland with few punctate calcifications and associated lytic changes of the adjacent left frontal bone that are suggestive of tumor recurrence C. Four months post-op after repeat orbitotomy and debulking of tumor with chemotherapy
Discussion
This is a case of a 36-year-old, male who presented with Adenoid Cystic Carcinoma of the lacrimal gland. Because of the location of the lacrimal gland at the superotemporal region of the orbit, ACC often presents with proptosis associated with inferomedial globe dystopia and upper lid fullness or swelling, which were present in this case with a short duration of 3 months. The mass of ACC typically lacks a surrounding capsule, extends into the posterior orbit and may exhibit pain from bone and perineural invasion.
On imaging, this tumor may have irregular borders with bony erosion and in some cases, may present focal calcification. Some authors attempted to correlate histologic subtype and its poor prognosis. Lee et al. found that a better prognosis was noted among cribriform variants or those with ‘Swiss cheese’ pattern. 5 In the study of Gamel and Font, they found a 5-year survival rate of 21% for patients with basaloid variant compared with 71% for patients with other variants. 6 This is in contrast to the study by Friedrich and Bleckmann, wherein they found that only tumor stage had statistically significant impact on prognosis. 7 The study of Ahmad and Esmaeli supported this, and wherein they concluded that prognosis was worse for patients with >T3 tumors, with a higher incidence of recurrence and metastasis despite aggressive treatment. 8 Our patient was initially staged T3aN1M0 and on 2nd year follow up, he had tumor recurrence and metastasis (T3aN1M1).
The treatment of ACC of the lacrimal gland is still controversial. Traditionally, its treatment is orbital exenteration followed by radiation therapy as supported by the study of Esmaeli et al. 9 Because orbital exenteration does not prevent a recurrence, relapse and death, Woo KL et al., found that eye-sparing surgery with eye-sparing radiation therapy offers preservation of visual function with good local control. 10 This study is supported by the study by Hung JY et al. but limited to diseases staged T1 or T2. 11 Despite surgery and radiation therapy, the prognosis for these patients remains poor. Some experts like Meldrum et al. incorporated neoadjuvant intracarotid cisplatin combined with intravenous doxorubicin into the conventional treatment for this disease. Among their 2 subjects, no recurrence was noted during their follow-up. 12 Tumor recurrence after tumor excision was seen in our case. He was initially advised post-operative radiotherapy however he was lost to follow up. Two years after the surgery, recurrence with intracranial extension was seen on imaging. Systemic work up showed lung metastasis. A globe-sparing approach was opted by our patient and a repeat lateral orbitotomy with debulking of the tumor was done. He has undergone chemotherapy with Cisplatin and oral Capecitabine.
Conclusion
ACC is a rare malignant tumor with poor prognosis correlating with the tumor variant and stage. Initially, our patient was staged T3aN1M0 but after 2 years after surgical removal he followed up with a tumor recurrence and a more aggressive stage T3aN1M1, for which he was managed with globe-sparing orbitotomy, surgical debulking and chemotherapy. Given the tendency of the disease for local and regional recurrence and metastasis despite treatment, close follow-up among these patients is critical.
References
- 1.Haque M N, ASM J Chowdhury, Ali M Y, Islam MMSU.Adenoid Cystic Carcinoma of the Lacrimal Gland Metastasizing after a Short Follow-up to Multiple Distant Bones - a Case Report with a Review of the Literature. Faridpur Med. , Coll. J 10(2), 84-86.
- 2.Ng Jacqueline.. , Adenoid Cystic Carcinoma of the Lacrimal Gland.https://eyewiki.aao.orgAdenoid_Cystic_Carcinoma_of_the_Lacrimal_Gland
- 3.Cantor. (2016) Basic and Clinical Science Course, Section 7: Orbit, Eyelids, and Lacrimal System, American Academy of Ophthalmology. , San Francisco
- 4.Francisco P Bernardini, Martin H Devoto, Oscar J.Croxatto. Epithelial tumors of the lacrimal gland: an update. Current Opinion in Ophthalmology 2008, 19: 000 – 000, ß 2008 Wolters Kluwer Health | Lippincott , Williams .
- 5.Lee D A, Campbell R J, Waller R. (1985) A clinicopathologic study of primary adenoid cystic carcinoma of the lacrimal gland. Ophthalmology. 92, 128-134.
- 6.Gamel J W, Font R L. (1982) Adenoid cystic carcinoma of the lacrimal gland: the clinical significance of a basaloid histologic pattern. Human Pathol. 13, 219-225.
- 7.Friedrich R E, Bleckmann V. (2003) Adenoid cystic carcinoma of salivary and lacrimal gland origin: localization, classification, clinical pathological correlation, treatment results and long-term follow-up control in 84 patients. Anticancer Res. Mar-Apr;23(2A): 931-40.
- 8.Bartley G, Harris G J. (2002) Adenoid cystic carcinoma of the lacrimal gland: Is there a cure…yet? Ophthal Plast Reconstr Surg. 18(5), 315-8.
- 9.Esmaeli B, Golio D, Kies M, DeMonte F. (2006) Surgical management of locally advanced adenoid cystic carcinoma of the lacrimal gland. Ophthalmic Plast Reconstr Surg. 22(5), 366-70.
- 10.Woo K I, Kim Y D, Sa H S, Esmaeli B. (2016) Current treatment of lacrimal gland carcinoma. Curr Opin Ophthalmol. 27(5), 449-56.