
Abstract
This study investigated the healthcare provider’s knowledge and attitudes towards induced abortion in Rwanda. A total of 152 healthcare providers from six public hospitals in Kigali city participated in this study. Questionnaires were used to record data on demographics, level of knowledge and attitudes towards abortion law then be cleaned, coded and entered into Excel sheet. Then all data were exported into SPSS version 22 for final cleaning and analysis. The study findings revealed that 54.6% were female, 56.0% were single, and 73% participants said that they attended formal training on abortion care. The study findings revealed that 23.70% healthcare providers had poor knowledge towards legal abortion law, and 57.20% had positive attitude with regards to induced abortion law. The findings revealed that religion and formal training on abortion care were among the factors which were strongly influencing attitudes of health care providers towards induced abortion where protestants were unlikely to have positive attitude with regards to induced abortion (AOR=0.277; 95% CI=0.027-0.377; P=<0.001) compared to participants belonged to catholic religion and participants who were not trained were unlikely to have positive attitude with regards to induced abortion (AOR=0.696; 95% CI=0.056-0.721; P=0.048) compared to trained respondents. It concludes that marital status, category of caregiver, religion, formal training on abortion and level of knowledge were the main risk factors of level of attitude towards induced abortion. More training about induced abortion are highly needed among health care providers to increase related knowledge as well as to eliminate negative attitude towards induced abortion.
Author Contributions
Academic Editor: Anubha Bajaj, Consultant Histopathologist
Checked for plagiarism: Yes
Review by: Single-blind
Copyright © 2022 Jean Paul Ndayizeye, et al.
 This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Competing interests
The authors have declared that no competing interests exist.
Citation:
Introduction
In 2017, the WHO reported that clandestine abortions keep being meaningful cause of maternal mortality and morbidity globally. It was counted that; worldwide over 56 million induced abortions occurred within a period of 2010–2014. In developed countries, reports highlighted a significant decline in abortions between 1994 and 2014. In fact, all causes abortions represented 39% and 27% of all pregnancies, respectively. However, developing countries still struggled with increasing abortion rates in the same period. Abortion rates increased from about 21% to 24% between 1994 and 2014 1.
In least developed nations with more prohibitive abortion laws, safe and medical induced abortion is not always accessible to women and girls having even sometimes-legal authorization. Despite the utmost important place of health care professionals in providing legalized abortion care services, their shortfall and lack of willingness to do so constitute the main challenges for abortion services 2.
According to the WHO 2016 report, of about 4.2 million women who underwent clandestine abortion in Africa and each year, nearly 1% lost their lives due to abortion-related complications. For example, Kenya has registered an estimated 464,000 induced abortions for only 2012 with almost a ratio of 30 abortions over 100 live births 3. Uganda also recorded an estimated 314,304 induced miscarriages in 2013, slightly above 110,000 and 294,000, respectively in 2003 4.
In Brazil, there are already ample knowledge on induced abortion and medical professionals, whereby a study done on 572 obstetrician-gynecologists only 48% reported accurate knowledge on abortion law 5. Another study done in Guatemala to identify both clinical and legal knowledge among obstetrician and gynecologists revealed that only 73% of them recognized that a legal abortion is granted when the life of woman is in danger following pregnancy 6.
In Ghana, where also abortion is allowed under certain circumstances, a study revealed that, most of midwives were not able to show a good understanding of abortion law and some had a wrong interpretation of the nature of abortion law 7. In Zimbabwe where legal abortion limited only 25% of HCPs recognized all four reasons under when abortion is allowed and about 31% were not informed about one or more legal grounds 8.
However, seen in some cases that health care professionals are conversant with legal abortion laws in their countries some are left behind. This can be seen in a study conducted in Argentina where the health care providers had not gotten sufficient knowledge on legal abortion policies within the country 9.
A study conducted among 405 mid-level healthcare providers 71.9% knew the contextualized definition of legal abortion in Ethiopia, 81.5% of them were conversant with the revised abortion law and only 53.1% of them had good knowledge on medical abortion care and only 54.1% of them had positive attitude towards safe abortion. Another study done in Ethiopia revealed that almost 54.1% mid-level HCPs had positive attitude towards medical abortion, and furthermore, HCPs with sufficient knowledge on medical abortion and male providers were more likely to show positive attitude with regards to medical abortion 10.
In the USA, a study was done on 278 physicians working in SHR services. Almost all strongly agreed that abortion can be provided in cases of pregnancy resulted from rape (89.6%), incest (89.2%), health risk (91.0%), and fetal abnormality (85.9%) 11.
In Ethiopia, it has been seen that healthcare providers have a more favorable views and attitude towards the providing safe abortion services, which is partially promoted due to an enabling environment. The result is that the majority of HCPs had a positive attitude towards medical abortion services 12.
Furthermore a greater number of health care providers (67.3%) had unfavorable attitudes towards induced abortion in Pakistan 13. Almost same results were found in India whereby 62% of the HCPs had positive attitude with regards to medical abortion care provision 14.
In Mexico about (71.1%) of healthcare providers supported abortion under certain circumstances and specifically, the majority (88.8%) support induced abortion for grounds where the pregnancy place at risk the life of the mother, when pregnancy results from rape (83.5%), and in case of fetal anomalies (83.5%) 15.
On the other hand in Zimbabwe, most healthcare providers were in support of liberalizing abortion law specifically to grounds when the pregnancy place risk of mother’s life (65%) and in cases when a mother is mentally handicapped (66%) 8. In Brazil and Zambia, evidences showed a lack of willingness for provision of medical abortion among some medical professionals and to some extend women who do not demonstrate medical conditions 16, 17.
The 1977 Rwanda abortion legislation restricted abortion; this was allowed only while preserving the health of a woman. In fact, abortion was illegal. Back in 2012, Rwanda approved abortion legislation and abortion was permissible in following cases of incest, rape, forced marriage and when there is a health-related problem either for pregnant woman or the fetus.
Since 2012 till later 2018, to obtain a legal abortion; a woman or girls looking for abortion was supposed to bring a certification from a “competent Court” explaining that the pregnant was resulted from incest, rape, or in forced marriage. To obtain a legal abortion because women/girls health related issue, one must get permission from two doctors with a written report in three copies
Despite restrictive abortion legislation in Rwanda, nearly 60,000 induced abortions were registered from 2009 to 2012, with a rate of 25 abortions per 1,000 women and girls aged between 15 to 44 years over one year 18.
Recently in 2019, a ministerial order was released in the official Gazette no.14 of 08/04/2019 removing those pre-conditions of obtaining a court order and two doctors’ approval in order to access a safe abortion. Now, one doctor can perform abortion without requiring court order only in following cases: when the pregnant person is a child; in case of rape; in case pregnant woman was subjected to a forced marriage, in case of pregnancy resulted from incest pledged with a man to the second degree of kinship, and lastly when the pregnancy present a risk to the health of the mother or to the foetus.
Kigali, the nation’s capital, registers a disproportionate figures of abortions relative to its total population; almost one-third of country’s abortions cases occur in Kigali city, although its host only one-tenth of the Rwanda’s women and girls of reproductive age 18. As front-line, health care providers (nurses, midwifes and doctors) working in obstetrics and gynecology department have most important role in the exertion of Rwanda legal abortion, therefore, promoting women and girls’ sexual reproductive health and rights. Talking abortion services provision in Rwanda, it is extremely meaningful to explore and have an idea on health care service provider’s perspectives on such services especially after new abortion law has been released 2019.
The present study investigated health care providers’ knowledge and views that shape the provision of abortion services. The results from this study enabled the country understand provider opinions on abortion and their implications policy implementation.
Methods
Research Design
The study used cross-sectional and quantitative approaches with the aim to investigate healthcare providers’ level of knowledge on current abortion law. Here, the goal was to found out beliefs of individuals on the nature of a particular phenomenon 19. This design was appropriate in this case because health care providers are a group of individuals who may have different knowledge, experiences and thoughts as far as induced abortion was concerned which needs to be understood and meanings brought out of the topic for public health purpose.
Research Setting
The study was conducted in Kigali City within 6 public hospitals of Kigali city: Kigali University Teaching Hospital, Muhima District Hospital, Kacyiru District Hospital, Kibagabaga District Hospital, Masaka district hospital and Rwanda Military Hospital. The Kigali city has women fertility rate of 3.6%, which is the least compared to other provinces of Rwanda (RDHS 2014/15).
The city has higher rates of unplanned pregnancies resulting to clandestine abortion and consequently 18 cases per 1,000 women who had abortion being treated for complications 18. The greatest proportion of hospitals rendering specialized health services related to obstetrics is in this city and mainly public health facilities.
Target Population
The research included medical providers working in maternity units from the 6 public hospitals of Kigali city which includes: Kigali University Teaching Hospital, Muhima District Hospital, Kacyiru District Hospital, Kibagabaga District Hospital, Masaka district hospital and Rwanda Military Hospital. Study participants were nurses, doctors, and midwives of all age group, educational qualification, and gender. The diversity of this group allowed the researcher to adequately exploring the knowledge and attitudes of those providers on the abortion for health purposes. Approximately 300 healthcare providers (nurses, doctors, and midwives) work in the targeted hospitals.
Sample Size and Sampling Procedure
At the beginning, a random sampling was used to select study participants out of the population size. The sample size was stratified and we used 2 subgroups such as medical doctors and nurses/midwives. The total population is made of 100 medical doctors and 200 nurses/midwives making approximately 33.3% and 66.7% proportions respectively. Therefore, those proportions were applied to our sample population and there were 50 medical doctors and 102 nurses/midwives study participants. Further stratification was done according to the health facilities included (6 hospitals) and according to the total of 300 healthcare providers included (60 health care providers from Kigali University Teaching Hospital, 50 healthcare providers from Muhima District Hospital, 50 healthcare providers from Kacyiru District Hospital, 44 healthcare providers from Kibagabaga District Hospital, 40 healthcare providers from Masaka district hospital and 56 healthcare providers Rwanda Military Hospital). The proportions of total sample size were as follow; 31 health care providers from Kigali University Teaching Hospital, 25 healthcare providers from Muhima District Hospital, 25 healthcare providers from Kacyiru District Hospital, 22 healthcare providers from Kibagabaga District Hospital, 20 healthcare providers from Masaka district hospital and 29 healthcare providers Rwanda Military Hospital making a total of 152 participants.
Data Collection
Data were collected using structured questionnaire, which was conceptualized, based on research objectives to answers each of research questions. This research questionnaire contained the dependent variable and independent variables that enabled researcher to determine the level of knowledge and attitude of health care providers as well as to answer the last research question, which consists of factors influencing providers’ attitude towards induced abortion in Kigali city, Rwanda.
Data Analysis
Data analysis was done using quantitative methods; questionnaires were cleaned, variables were coded and launched into Excel sheet. Categorical data on knowledge on abortion law among healthcare providers (Yes, No and I don't know) were classified as good knowledge (above the mean) or poor knowledge (less than the mean). On the other hand, categorical data on attitudes of healthcare providers towards induced abortion (Agree and Disagree) were classified as positive attitude (above the mean) and negative attitude (less than the mean).
All data was then exported to SPSS version 22 for final cleaning and analysis. A descriptive analysis of demographic information was performed to identify frequency distributions, proportions, and proportions of participants. The chi-square test was performed to determine the association between categorical variables (knowledge and attitude demographics). Finally, we used logistic regression to determine the association between the dependent and independent variables with 95% confidence intervals.
Ethical Consideration
At the beginning of the study, the data collection authorization letter was given by Mount Kenya University. Prior to data collection, research respondents were communicated the nature and sensitivity of the research and further ethical clearances were obtained from Hospital ethics committees where existing. Anonymity and confidentiality maintained and respondents protected by not disclosing any information potentially linked to them. All participants were informed that they allowed quitting from the study anytime they are not confortable with it. Due to the sensitivity of the information that was provided by the health care providers, the researcher ensured study participants that the information is only used for research purposes only, and no personal information that was link to the respondents were disclosed.
Results
Socio-Demographic Characteristics of Respondents
As indicated in table 1 below, those are socio-demographic characteristics of 152 respondents all reached and data collected using questionnaire through face-to-face interview.
The table 1 shows that 69(45.4%) were male and 83(54.6%) were female. For marital status, the higher number of participants were single with a total number of 84(56.0%) and married participants were 68(44.0%). 111(73%) participants said that they attended formal training on abortion care, 62(40.8%) were midwives and 39(25.7%) were nurses. The majority of the participants 100(65.8%) had the duration ranging between 1-10 years in medical practices and the few number of only 11 participants had been in medical practices for over twenty years.
Table 1. Socio-demographic characteristics of respondents| Variables | Frequency | Percentage (%) |
|---|---|---|
| Age in range | ||
| 20-30 Years | 38 | 25 |
| 31-40 Years | 78 | 51.3 |
| >40 years | 36 | 23.7 |
| Gender | ||
| Male | 69 | 45.4 |
| Female | 83 | 54.6 |
| Marital status | ||
| Married | 68 | 44 |
| Single | 84 | 56 |
| Religion | ||
| Catholic | 69 | 45.4 |
| Protestant | 83 | 54.6 |
| Formal training on abortion care | ||
| Yes | 111 | 73 |
| No | 41 | 27 |
| Healthcare provider category | ||
| GP | 25 | 16.4 |
| GO Specialist | 17 | 11.2 |
| GO Resident | 9 | 5.9 |
| Midwife | 62 | 40.8 |
| Nurse | 39 | 25.7 |
| Duration in medical practice | ||
| 1-10 Years | 100 | 65.8 |
| 11-20Years | 41 | 27 |
| >20Years | 11 | 7.2 |
Healthcare Providers’ Level of Knowledge on Rwandan Legal Abortion Law
The objective one was to determine HCPs’ level of knowledge on Rwandan legal abortion law and was measured by score assessment of thirteen variables.
Among the participants, 148(97.4%) of them agreed that they knew that there is abortion legislation in Rwanda, 101(66.0%) participants said that all medical doctors are granted to provide abortion services and 136(89.9%) of them were agreed with the statement which was asking if abortion is allowed when a child aged less than 18 years. 130(85.5%) of respondents agreed with the statement which was asking whether abortion is allowed in case to pregnant person with forced marriage while 131(86.2%) of them were not agree with the statement which was asking if abortion is allowed in case of the person who requesting for it can’t afford a child. (Table 2)
Table 2. Level of knowledge on Rwandan legal abortion law| Variables | Frequency | Percent |
|---|---|---|
| Do you know that there is abortion legislation in Rwanda? | ||
| No | 4 | 2.6 |
| Yes | 148 | 97.4 |
| Legal abortion is defined as termination of pregnancy under grounds allowed by the law | ||
| Yes | 120 | 78.9 |
| No | 22 | 14.5 |
| I don't know | 10 | 6.6 |
| All recognized medical doctors working either in governmental or in private health institutions are granted to provide abortion services | ||
| Yes | 101 | 66.4 |
| No | 35 | 23 |
| I don't know | 16 | 10.5 |
| A person asking for abortion is not required to provide evidence | ||
| Yes | 64 | 42.1 |
| No | 76 | 50 |
| I don't know | 12 | 7.9 |
| Abortion is allowed for a child aged less than 18 years | ||
| Yes | 136 | 89.5 |
| No | 13 | 8.6 |
| I don't know | 3 | 2 |
| Abortion can be performed at any gestational age provided that the person requesting abortion presents with a ground by which abortion is allowed by the law | ||
| Yes | 20 | 13.2 |
| No | 129 | 84.9 |
| I don't know | 3 | 2 |
| Abortion is allowed in case a pregnancy has resulted from rape? | ||
| Yes | 139 | 91.4 |
| No | 8 | 5.3 |
| I don't know | 5 | 3.3 |
| Abortion is allowed in case of the pregnant person became pregnant secondary to a forced marriage | ||
| Yes | 130 | 85.5 |
| No | 15 | 9.9 |
| I don't know | 7 | 4.6 |
| Abortion is allowed in case of the pregnant person became pregnant secondary to incest committed with a man from the second degree of kinship | ||
| Yes | 131 | 86.2 |
| No | 12 | 7.9 |
| I don't know | 9 | 5.9 |
| Abortion is allowed in case a pregnancy place at risk the health of the mother or the foetus | ||
| Yes | 147 | 96.7 |
| No | 5 | 3.3 |
| Abortion is allowed in case of the person requesting for abortion is mentally incapable | ||
| Yes | 62 | 40.8 |
| No | 66 | 43.4 |
| I don't know | 24 | 15.8 |
| Abortion is allowed in case of the person requesting abortion can’t afford to care a child | ||
| Yes | 17 | 11.2 |
| No | 131 | 86.2 |
| I don't know | 4 | 2.6 |
| Abortion is allowed in case of the person requesting abortion is a girl and still in school | ||
| Yes | 20 | 13.2 |
| No | 126 | 82.9 |
| I don't know | 6 | 3.9 |
The Score of Level of Knowledge on Rwandan Legal Abortion Law
The overall score is 13 and its mean is 9.60. The scores are 0 and 1 for No and Yes respectively and the results are presented in Figure 1. The participants with score less than the mean score, considered to have poor knowledge and the one with score greater than mean had good knowledge.
Figure 1.Level of knowledge
The study findings revealed that the majority of health care providers in Kigali of 116(76.30%) had good knowledge towards Rwandan legal abortion law and few of respondents 36(23.70%) had poor knowledge towards Rwandan legal abortion law.
Attitudes Towards Induced Abortion Law Among Health Care Providers in Kigali.
The objective two was to assess attitudes towards induced abortion law among HCPs and was also measured by score assessment of six variables.
For assessing an attitude of health care providers in Kigali, six statements have been used. Among the participants, 96(63.2%) of them agreed the statement that was asking whether they agree with any of the grounds under which abortion is allowed in Rwanda and 93(61.2%) supported the statement saying that the abortion done when the person who looking for it is aged under eighteen. For the statement that was asking whether abortion is allowed in case of the person who asking for abortion wasraped, 54(35.5%) of the respondents did agree that statement while 143(94.1%) of respondents agreed the statement asked whether the abortion should be done in case of thepregnancy place at risk the health of the mother. (Table 3)
Table 3. Attitude towards induced abortion law| Variables | Frequency | Percent |
|---|---|---|
| Do you agree with any of the grounds under which abortion is allowed in Rwanda? | ||
| I agree | 96 | 63.2 |
| I disagree | 56 | 36.8 |
| Do you agree that abortion could be provided in case of the pregnant person is a child aged less 18year? | ||
| I agree | 93 | 61.2 |
| I disagree | 59 | 38.8 |
| Do you agree that abortion could be provided in case pregnancy resulted from a rape? | ||
| I agree | 98 | 64.5 |
| I disagree | 54 | 35.5 |
| Do you agree that abortion could be provided in case pregnancy resulted from a forced marriage? | ||
| I agree | 89 | 58.6 |
| I disagree | 63 | 41.4 |
| Do you agree that abortion could be provided in case of the pregnant person became pregnant secondary to incest committed with a man from the second degree of kinship? | ||
| I agree | 91 | 59.9 |
| I disagree | 61 | 40.1 |
| Do you agree that abortion could be provided in case of the pregnancy place at risk the health of the mother or the foetus | ||
| I agree | 143 | 94.1 |
| I disagree | 9 | 5.9 |
The Score of Attitude Towards Induced Abortion Law.
The overall score is 6 and its mean is 4.01. The scores are 0 and 1 for I disagree and I agree respectively and the results are presented in Figure 2. The participants with score less than the mean score, considered to have negative attitude and the one with score greater than mean had positive attitude.
Figure 2.Attitude towards induced abortion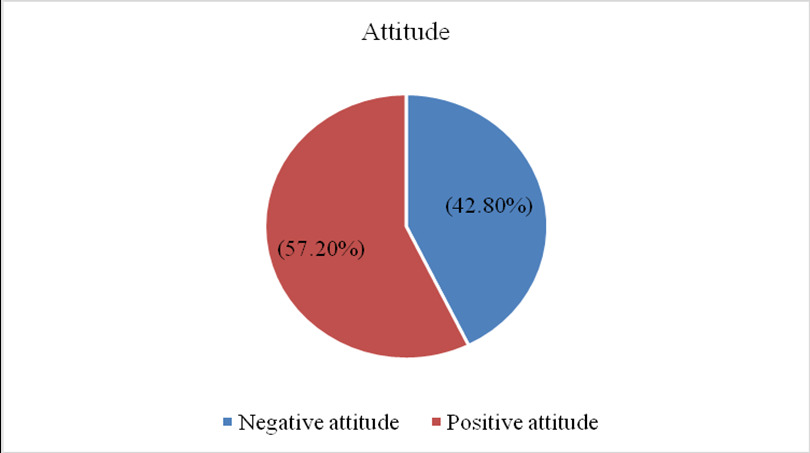
The study findings showed that over a half of HCPs 87(57.20%) had positive attitude towards induced abortion law and 65(42.80%) HCPs had negative attitude towards induced abortion law.
Factors Influencing Attitudes of Health Care Providers Towards Induced Abortion in Kigali
Objective three was to determine factors influencing attitudes of healthcare providers towards induced abortion in Kigali and was calculated by using the assessment of variables presented in table 4 below. In order to determine these factors influencing healthcare providers’ attitudes towards abortion in Kigali city, a cross-tabulation was done to test any possible association between independent variables (demographics and level of knowledge) and dependent variable (attitude towards induced abortion).
Table 4. Factors influencing attitudes of healthcare providers towards induced abortion in Kigali| Variables | AOR | 95%CI | P-value | |
|---|---|---|---|---|
| Lower | Upper | |||
| Marital status | ||||
| Married | Ref | |||
| Single | 0.693 | 0.32 | 1.503 | 0.353 |
| Healthcare provider category | ||||
| GP | Ref | |||
| GO Specialist | 1.991 | 0.575 | 6.897 | 0.277 |
| Midwife | 1.314 | 0.334 | 5.175 | 0.696 |
| Nurse | 0.863 | 0.346 | 2.152 | 0.752 |
| Religion | ||||
| Catholic | Ref | |||
| Protestant | 0.277 | 0.027 | 0.377 | <0.001 |
| Formal training on abortion care | ||||
| No | 0.696 | 0.056 | 0.721 | 0.048 |
| Yes | Ref | |||
| Level of knowledge | ||||
| Poor knowledge | 0.752 | 0.752 | 0.752 | 0.11 |
| Good knowledge | Ref | |||
Multivariate analysis was performed in this study to check how strong association was between variables.
Findings revealed that the religion was among the factors which was strongly influencing attitudes of HCPs towards induced abortion where protestants were unlikely to have positive attitude with regards to induced abortion (AOR=0.277; 95% CI=0.027-0.377; P=<0.001) compared to participants belonged to catholic religion. Formal training on abortion care, shown to be the factor influencing attitudes of HCPs towards induced abortion where participants who were not trained were unlikely to have positive attitude with regards to induced abortion (AOR=0.696; 95% CI=0.056-0.721; P=0.048) compared to trained respondents.
Discussion
This study intended to investigate healthcare provider’s knowledge and attitudes towards induced abortion in public hospitals of Kigali city, Rwanda. The present study revealed that over a half of healthcare providers 76.3% had good knowledge and 57.20% had positive attitude towards induced abortion law.
Healthcare provider’s knowledge about abortion law in Rwanda is almost the same compared to that reported in a study conducted in Ethiopia where only 71.9% healthcare providers knew the definition of abortion, 53.1% of them had sufficient knowledge on medical abortion and about 81.5% of them were conversant with the country’s abortion law 10. This was also the same for healthcare providers in Guatemala whereby 73% of obstetrician and gynecologists recognized that legal abortion is granted in case pregnancy place woman's life is at risk 6. The similarities in percentages maybe explained that in the two studies conducted in both Ethiopia and Guatemala have mostly included more midwives and obstetrician and gynecologists who maybe always familiar with abortion law even from their usual training.
On the other hand, healthcare provider’s knowledge about abortion law in Rwanda was higher compared to Brazilian medical professionals where only 48% medical professionals out of 572 obstetrician-gynecologists reported accurate knowledge on abortion law 5. This was also much higher than in Zimbabwe where only 25% of healthcare providers knew all four reasons under which abortion is legal and about 31% were not informed about one or more legal grounds 8.
The different in percentages of health care providers with good knowledge in Rwanda and the two countries; Zimbabwe and Brazil, maybe linked with the differences in terms of abortion legislations in these countries. Both Brazil and Zimbabwe have very restrictive abortion laws that only permit abortion in cases of rape, fetal abnormalities, or risk to life of the mother.
The present findings revealed that over a half of health care providers 57.20% had positive attitude towards induced abortion law and 42.80% health care providers had negative attitude towards induced abortion law. The level of attitude was assessed by asking the questions related to an induced abortion law in Rwanda, where the respondents would answer the questions by supporting or not supporting each of the grounds under which abortion is allowed in Rwanda.
These findings were in the line with other three studies done in Ethiopia, India and Mexico where by almost 54.1% mid-level healthcare providers in Ethiopia had positive attitude towards safe abortion 10, in India about 62% HCPs were identified to have positive attitude with regards to medical abortion provision 14. Lastly in Mexico about (71.1%) of healthcare providers supported abortion 15.
On the other hand, the majority of health care providers in Pakistan (67.3%) had unfavorable attitudes towards induced abortion 13. This may be linked to the fact that Pakistan is a deeply conservative Muslim country and abortion is permitted only to save the woman’s life.
The most factors influencing healthcare providers’ attitudes towards induced abortion in Kigali generally are; marital status, category of caregiver, religion, formal training on abortion and level of knowledge. For the factors which influencing the attitude towards induced abortion, specifically religion and formal related training showed to be the factors with strong association with healthcare providers’ attitude towards induced abortion in Kigali.
The present study was in the same line with the study conducted from South Africa, which concluded that, both training on medical abortion and certification of midwives were identified as factors influencing positive attitude towards induced abortion and this led to a critical step during providing of quality medical abortion services. The same applied on the religion as one of the factor influencing attitude among health care providers, this study found out that religious, moral beliefs and fears contributed much in taking decision of being involved in an induced abortion 20.
Religion was also one of the key factors influencing healthcare providers’ attitude towards abortion care in Ethiopia 21. Another study conducted in Adama, Ethiopia, among HCPs who were opposed the abortion law, religion, cultural norms and lack training on medical abortion were the main factors influencing their attitudes towards induced abortion 22.
Conclusion
The study’s aim was to investigate healthcare provider’s knowledge and attitudes towards induced abortion in public hospitals of Kigali city, Rwanda.
The finding of this study revealed that that the majority of health care providers in Kigali had good knowledge towards Rwandan legal abortion law and lower percentage of respondents had poor knowledge towards Rwandan legal abortion law. Although, this study revealed marital status, category of caregiver, religion, formal training on abortion and level of knowledge were the main risk factors of level of attitude towards induced abortion.
The result can’t be generalized for whole country in consideration of the study design, sample size and the characteristics of study population (health care providers) in urban area that can differ from those characteristics in rural. Further studies including qualitative methods related to abortion law in Rwanda in Kigali and even countrywide is recommended as we are still having a high number of clandestine abortions.
References
- 1.onda Tsuyoshi, SSLRGSLK. (2017) Uneven Progress and Unequal Access. Abortion Worldwide 2017: Uneven Progress and Unequal Access. 1-68.
- 2.U R Loi, Gemzell-danielsson K, Faxelid E, Klingberg-allvin M. (2015) Health care providers ’ perceptions of and attitudes towards induced abortions in sub-Saharan Africa and Southeast Asia a systematic literature review of qualitative and quantitative data.BMC Public Health.https://doi.org/10.1186/s12889-015-1502-2.
- 3.S F Mohamed, Izugbara C, A M Moore, Mutua M, E W Kimani-Murage et al. (2015) The estimated incidence of induced abortion in Kenya: A cross-sectional study. , BMC Pregnancy and Childbirth 15(1), 1-10.
- 4.Prada E, L M Atuyambe, N M Blades, J N Bukenya, C G Orach et al. (2016) Incidence of induced abortion in Uganda, 2013: New estimates since 2003.PLoSONE,11(11). 1-19.
- 5.L A Goldman, S G García, Díaz J, E A Yam. (2005) Brazilian obstetrician-gynecologists and abortion: A survey of knowledge, opinions and practices. Reproductive Health. 2(1), 1-9.
- 6.Kestler E. (2012) Obstetrician-gynecologists’ knowledge of and attitudes toward medical abortion in Guatemala. , International Journal of Gynecology and Obstetrics 116(2), 120-123.
- 7.Oppong-darko P, Amponsa-achiano K, Darj E. (2017) I Am Ready and Willing to Provide the Service. Though My Religion Frowns on Abortion”— Ghanaian Midwives Mixed Attitudes to Abortion Services: A Qualitative Study.International Journal for Environmental Research and Public Health.
- 8.Madziyire M G, Moore A, Riley T, Sully E, Chipato T. (2019) Knowledge and attitudes towards abortion from health care providers and abortion experts in zimbabwe: A cross sectional study. , Pan African Medical Journal 34.
- 9.Ramos S, Romero M, Michel Ramón, A. (2014) Health care providers’ opinions on abortion: A study for the implementation of the legal abortion public policy in the Province of Santa Fe, Argentina. Reproductive Health. 11(1), 1-10.
- 10.E M Assefa. (2019) Knowledge, attitude and practice (KAP) of health providers towards safe abortion provision. in Addis Ababa health centers.BMC Women’s Health,19(1) 1-10.
- 11.L E Dodge, Haider S, M R Hacker. (2016) Attitudes toward Abortion among Providers of Reproductive Health Care.Women’s Health Issues,26(5). 511-516.
- 12.Abdi J, M B Gebremariam. (2011) Health providers’ perception towards safe abortion service at selected health facilities in Addis Ababa. , African Journal of Reproductive Health 15(1), 31-36.
- 13.B R Crisp, Federation W, Medical F O R, Forsetlund L, Bjørndal a et al. (2013) . Attitudes of Health Care Providers to Induced Abortion in Pakistan. Journal of the College of Physicians and Surgeons--Pakistan JCPSP 21(2), 124.
- 14.Pyne S, Ravindran T K S. (2020) Availability, Utilization, and Health Providers’ Attitudes Towards Safe Abortion Services in Public Health Facilities of a District in West Bengal, India. Women’s Health Reports. 1(1), 80-88.
- 15.García-Núñez N N, Atienzo E E, Dayananda I, Walker D. (2013) Legislation, knowledge and attitudes of health professionals in Mexico regarding abortion. Salud Colectiva. 9(2), 235-246.
- 16.D B Cacique. (2011) knowledge, and attitudes of health professionals on inducedabortion review. of Brazilian studies ( 2001-2011 )Opiniões,conhecimentoeatitudesdeprofissionaisdabrasileiraspublicadasentre .
- 17.Berer M. (2002) Making abortions safe: A matter of good public health policy and practice. Reproductive Health Matters. 10(19), 31-44.
- 18.Basinga P, Moore A, Singh S, Remez L. (2012) Unintended Pregnancy And Induced Abortion In. Rwanda.Guttmacher Institute 2-32.
- 19.Z Q Al-busaidi. (2008) . Qualitative Research and its Uses in Health Care.SultanQuboosUniversity Medical Journal,8(1) 11-19.
- 20.Harries J, Stinson K, Orner P. (2009) Health care providers’ attitudes towards termination of pregnancy A qualitative study. in South Africa.BMC Public Health,11 1-11.