
Abstract
Objective
Investigate the effect of connecting a waterproof device at the front end of the piezometric tube on pressure transmission and patient-machine synchronization during the noninvasive ventilation.
Method
In test 1, the waterproof device was connected to the piezometric tube and put into a closed container, the pressure inside the container was varied to observe the corresponding pressure change in the piezometric tube. In test 2, a waterproof device was connected in front of the piezometric tube during noninvasive ventilation.12 subjects were received noninvasive ventilator so that dynamic changes of the pressure inside the mask (Pmask) and piezometric tube (Ptube) could be measured.
Results
In test 1, when the pressure in the container was gradually increased to 50 cmH2O and then decreased to 0, the pressure inside the piezometric tube changed synchronously with the pressure inside the container, with no statistically significant difference between the pressures (0.009 ± 0.138) cmH2O. In test 2, there was no significant increase in triggering time, pressure, and power after connecting the waterproof device at the front end of the piezometric tube. There was no significant difference in the platform pressure and baseline pressure as measured by Pmask, before and after connecting the waterproof device. Finally, there was no significant difference in the platform pressure and baseline pressure between Pmask and Ptube after connecting the waterproof device.
Author Contributions
Academic Editor: Ji X, Zhejiang University
Checked for plagiarism: Yes
Review by: Single-blind
Copyright © 2017 Hu Jieying
 This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Competing interests
The authors have declared that no competing interests exist.
Citation:
Introduction
Noninvasive positive pressure ventilation (NPPV) has been widely used in clinical and family rehabilitation. Since being developed, noninvasive ventilation has played an important role in treating acute and chronic respiratory failure1, 2, 3, 4. Compared with invasive mechanical ventilation, it has the advantage of being implemented at any time according to the requirements of the disease. In addition, ventilator-associated pneumonia and other serious complications are significantly reduced.5, 6
However, poor patient-machine synchronization is one of the major reasons why patients are reluctant to undergo noninvasive ventilation 7, 8, which affects clinical application of the technique. There are many factors that affect patient-machine synchronization, but the factors with clinical significance are patient factors, ventilator performance, respiratory parameters, ventilation mode, and leakage 9, 10, 11.
However, in clinical practice, patient-machine asynchrony caused by condensate in the piezometric tube during noninvasive ventilation may occur. The condensate obstructs the pressure transfer to the ventilator, leading to abnormalities of the ventilator and ventilation failure. To prevent condensate from entering the piezometric tube, a waterproof device was developed and connected to the opening of the tube. The effect of connecting the waterproof device at the front end of the piezometric tube on patient-machine synchronization during noninvasive ventilation was then investigated.
Material and methods
I. Study subjects
7 males and 5 females aged 24-52 years (31 ± 9 years) were recruited for the study. This test was approved by the Biomedical Ethics Committee of the First Affiliated Hospital of Guangzhou Medical University, and all volunteers gave informed consent.
II. Test equipment and data collection methods
1.Waterproof device: one end of an 0.8 cm long hollow cylindrical plastic pipe with a cross-sectional area of 1.3 cm2 was covered with a waterproof, breathable film, and the other end was connected to a piezometric tube (Figure 1).
Figure.1. Diagram of the waterproof device.
2. Pressure measurements: small tubes connected the mask and the loop piezometric tube to pressure sensors (P-300B type, Beijing Jinsanjiang Sensing Technology Co., Ltd.) for dynamic monitoring of Pmask and the pressure in the piezometric tube (Ptube) (Figure 1). The pressure signal was amplified through a PCLAB amplifier (3808 type, Guangzhou Yinghui Medical Devices Technology Co., Ltd.).
3. Ventilator model: a Curative FLEXOST-30 ventilator was used. Inhale positive airway pressure (IPAP) increased from 10 cmH2O to 30 cmH2O in 4 cmH2O increments, and exhale positive airway pressure (EPAP) from 4 cmH2O to 14 cmH2O in 2 cmH2O increments where 1 cmH2O = 0.098 kPa. The spontaneous breathing mode was used.
4. Data acquisition: acquisition frequencies for flow and pressure were 256 Hz. When all signals were amplified, a Powerlab 16-channel physiological recorder (ML796, ADInstruments, Australia) was used to log and analyse data via Chart5.2.1 software.
III. Connection methods
1. Connection method for test 1: tube A representing the piezometric tube connected the waterproof device to the container at one end to a pressure sensor at the other end; tube B connected the container at one end to a pressure sensor at the other end; and tube C connected the container to a pressure generator Figure 2.
Figure.2. Connection diagram for test 1.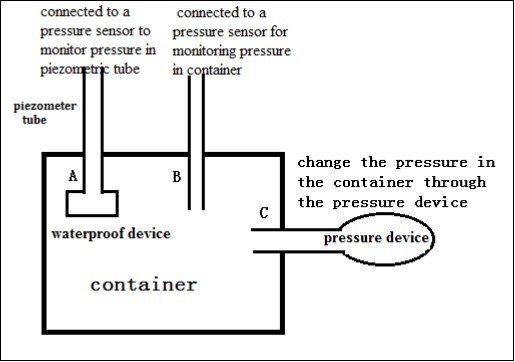
2. Connection method for test 2: The piezometric tube was connected with a waterproof device. The breathing channel and exhalation platform valve were connected between the mask and the ventilator Figure 3.
Figure.3. Connection diagram for test 2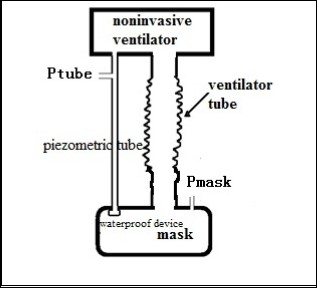
IV. Test steps
Test 1
the pressure generator gradually pressurized the sealed container to 50 cmH2O. The pressure was then gradually reduced to atmospheric pressure, and the changes in pressures inside the container and inside the piezometric tube were dynamically recorded.
Test 2
(1) the seated testers wore the mask, which was connected as shown in Figure 3, and the breathing circuit of the ventilator was connected to the exhalation platform valve, flow sensor, and mask.
(2) The IPAP/EPAP settings on the ventilator encompassed six different pressure states, namely, 10/4, 14/6, 18/8, 22/10, 26/12 and 30/14 cmH2O.
(3) At each pressure level, the dynamic changes in Pmask and Ptube were recorded for 3 minutes, before and after connecting the waterproof device at the front end of the piezometric tube.
(4) The data from 10 breathing cycles were taken before and after connecting the waterproof device at the front end of the piezometric tube to analyse differences in triggering times, pressure, power, and platform and baseline pressures based on Pmask and Ptube pressures.
V. Analysis of observation indexes
1. Triggering time was defined as the time between the initial drop in Pmask and when the air supply flow began (Figure 4).
2. Triggering pressure was defined as the pressure between the initial drop in Pmask and the drop-out value measured when the air supply flow began (Figure 4).
3. Triggering power was determined from the integral of the product of the triggering time and triggering pressure.
4. The average values determined the platform and baseline pressures.
Figure.4. Calculation diagram for triggering time and pressure.
VI. For statistical measures,
Statistical Program for Social Sciences 21.0 software (SPSS, Inc., Chicago, IL,USA) was used. Test results were expressed with the mean ± standard deviation, and the data among groups were compared by using the t-test, and P<0.01 indicated statistical significance.
Results
Test 1
The pressure difference between the piezometric tube and the container was (0.009 ± 0.138) cmH2O, and there was no significant difference between the two (P> 0.01) (Figure 5).
Figure.5. Bland-Altman diagram for pressure inside the container and piezometric tube.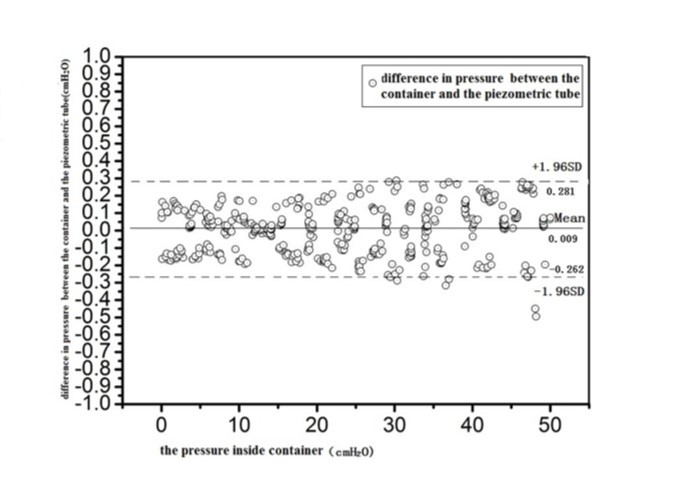
Test 2
(1) Before and after connecting the waterproof valve at the front end of piezometric tube, there were no significant statistical differences in the triggering time, pressure, and power (Table 1).
(2)There were no significant statistical differences in platform and baseline pressures measured via the mask, before and after connecting the waterproof valve at the front end of the piezometric tube (Table 1).
(3)There were no significant statistical differences in platform and baseline pressures between Pmask and Ptube , after connecting the waterproof valve at the front end of the piezometric tube (Table 1).
Table 1. The pressure and triggering situations before and after connecting a waterproof valve at the front end of piezometric tube| IPAP/EPAP | waterproof device | Platform pressure | Baseline pressure | Triggering time (S) | Triggering pressure (cmH 2 O) | Triggering power (cmH 2 O*S) | ||
| cmH2O | Pmask(cmH2O) | Ptube(cmH2O) | Pmask(cmH2O) | Ptube(cmH2O) | ||||
| 10-Apr | Yes | 10.03±0.11 | 10.00±0.09 | 3.96±0.14 | 3.96±0.11 | 0.08±0.03 | 0.62±0.25 | 0.06±0.03 |
| No | 9.90±0.63 | 9.91±0.63 | 3.96±0.04 | 3.99±0.04 | 0.08±0.04 | 0.62±0.34 | 0.06±0.04 | |
| 14-Jun | Yes | 13.93±0.12 | 13.91±0.10 | 5.96±0.10 | 5.95±0.08 | 0.09±0.02 | 0.70±0.42 | 0.09±0.08 |
| No | 13.94±0.10 | 13.95±0.08 | 5.97±0.05 | 5.97±0.05 | 0.08±0.04 | 0.69±0.36 | 0.08±0.04 | |
| 18-Aug | Yes | 17.91±0.09 | 17.90±0.11 | 7.89±0.09 | 7.89±0.07 | 0.09±0.03 | 0.79±0.41 | 0.09±0.07 |
| No | 17.90±0.17 | 17.90±0.14 | 7.91±0.06 | 7.89±0.05 | 0.09±0.04 | 0.76±0.40 | 0.09±0.05 | |
| 22-Oct | Yes | 20.58±0.72 | 20.57±0.71 | 9.88±0.07 | 9.87±0.07 | 0.10±0.03 | 0.84±0.43 | 0.09±0.07 |
| No | 20.76±0.78 | 20.73±0.79 | 9.89±0.09 | 9.86±0.08 | 0.10±0.04 | 0.85±0.31 | 0.09±0.07 | |
| 26-Dec | Yes | 21.31±1.19 | 21.30±1.19 | 11.80±0.08 | 11.81±0.09 | 0.10±0.03 | 1.05±0.47 | 0.11±0.08 |
| No | 21.57±1.05 | 21.53±1.06 | 11.81±0.11 | 11.80±0.12 | 0.09±0.04 | 0.98±0.41 | 0.10±0.06 | |
| 30/14 | Yes | 21.44±1.24 | 21.41±1.25 | 13.80±0.12 | 13.79±0.13 | 0.09±0.04 | 1.07±0.57 | 0.11±0.06 |
| No | 21.84±1.80 | 21.85±1.82 | 13.78±0.17 | 13.79±0.17 | 0.09±0.03 | 0.93±0.49 | 0.10±0.05 | |
Discussions
In the over 10 years of development, noninvasive ventilation has played an important role in aspects such as treating acute and chronic respiratory failure. However, because patients are often reluctant to accept noninvasive ventilation due in part to poor patient-machine synchronization the overall clinical use of this technique is adversely affected. Patient-machine synchronization in the spontaneously breathing patient requires the ventilation to respond to the patient’s inspiratory starting time and inspiratory-expiratory switching time. When they are asynchrous, the patient’s spontaneous respirations may oppose the ventilator breaths. This results in discomfort to the patient and failure of the noninvasive ventilator breaths to support the pulmonary needs of the patient 12. Therefore, there is an important clinical significance to improve the patient-machine synchronization for noninvasive ventilation.
The patient-machine synchronization of noninvasive ventilation is mainly manifested in three aspects: inspiratory trigger, pressure support level and inspiratory-expiratory switching 13, 14, which is realized through a piezometric tube in the noninvasive ventilation circuit: When the patient inhales, the Pmask drops and the ventilator starts to supply gas. During the gas delivery, the ventilator always adjusts the gas supply volume according to the Pmask feed back by the piezometric tube. When the pressure feed back is lower than preset value, the ventilator increases air volume and vice versa. Therefore, a piezometric tube plays a very critical role in the patient-machine interaction process.
However, in clinical practices, we often find the patient-machine asynchrony is caused by condensate in piezometric tube during noninvasive ventilation. The condensate leads to obstruction for the conduction of the mask pressure through the piezometric tube to the ventilator affecting the control of the ventilator supported breaths. In the previous study, we found that when the condensate is present in the piezometric tube (even if only 0.1ml), the pressure conduction times is prolonged and the pressure conduction decreases, which lead to patient-machine asynchrony situations: prolonged triggering, increased triggering pressure, enhanced triggering powers and unstable gas supply 15.
Therefore, we developed a waterproof device that connected at the front end of piezometric tube which is made of waterproof breathable membrane, and the membrane part is a hydrophobic material. It can prevent the condensate from entering piezometric tube without obstructing conduction of pressure.
From the results of test 1, we see that the pressure change is always consistent between piezometric tube and inside container after a waterproof device is connected at the front end of piezometric tube, and comparison between the two is not statistically significant (Figure 5). The results of Test 2 show that in noninvasive ventilation, the pressure of Ptube and Pmask always remains synchronized changing at different pressure support levels (the inspiratory pressure increased from 10cmH2O to 30cmH2O, and the expiratory pressure increased from 4cmH2O to 14cmH2O), with a waterproof device connected at the front end of piezometric tube. With a waterproof device connected at the front end of piezometric tube, the ventilator's gas supply is stable .There is no significant difference in Pmask with a waterproof device connected at the front end of piezometric tube comparing that situation with no waterproof device, and there is no significant difference in the triggering time, pressure and power.
In summary
In this study connecting a waterproof device at the front end of piezometric tube can prevent condensate from entering piezometric tube, which does not affect the pressure conduction and patient-machine synchronization of noninvasive ventilation.
References
- 1.Mal S, Mcleal S, lansavichene A. (2014) Effect of out-of-hospital noninvasive positive-pressure support ventilation in adult patients with severe respiratory distress: a systematic review and meta-analysis[J]. , Ann Emerg Med 63(5), 600-607.
- 2.Mas A, Masip J. (2014) Noninvasive ventilation in acute respiratory failure[J]. , Int J Chron Obstruct Pulmon Dis 9(1), 837-852.
- 3.Zhou L, Li X, Guan L, Chen J. (2017) Apr,27, Home noninvasive positive pressure ventilation with built-in software in stable hypercapnic COPD: a short-term prospective, multicenter, randomized, controlled trial[J].Int. , J Chron Obstruct Pulmon Dis 12, 1279-1286.
- 4.L Q Zhou, X Y Li, Li Y. (2016) Inspiratory muscle training followed by non-invasive positive pressure ventilation in patients with severe chronic obstructive pulmonary disease: a randomized controlled trial[J]. , Journal of Southern Medical University 36(8), 1069.
- 5.A M Meeder, D H Tjan, Zanten A R van. (2016) Noninvasive and invasive positive pressure ventilation for acute respiratory failure in critically ill patients: a comparative cohort study[J]. , Journal of Thoracic Disease 8(5), 813.
- 6.V A Maleh, Monadi M, Heidari B. (2016) Efficiency and outcome of non-invasive versus invasive positive pressure ventilation therapy in respiratory failure due to chronic obstructive pulmonary disease[J]. , Caspian Journal of Internal Medicine 7(2), 99-104.
- 7.Gilstrap D, Davies J. (2016) Patient-Ventilator Interactions[J]. Clinics in Chest Medicine. 37(4), 669-681.
- 8.Gilstrap D, Macintyre N. (2013) Patient-ventilator interactions, Implications for clinical management[J]. , American Journal of Respiratory & Critical Care Medicine 188(9), 1058.
- 9.Carteaux G, Lyazidi A, Crdoba-lzquierdo A. (2012) Patient-ventilator asynchrony during noninvasive ventilation: a bench and clinical study[J]. , Chest 142(2), 367-376.
- 10.Mellott K G, Grap M J, Munro C L. (2014) Patient ventilator asynchrony in critically ill adults: frequency and types[J]. , Heart Lung 43(3), 231-243.
- 11.Rodrigues G G, Aguirre C A, Cuvelier A. (2011) Global models for patient-ventilator interactions in noninvasive ventilation with asynchronies[J].Comput. , Biol Med 41(5), 253-264.
- 12.S K Epstein. (2011) How often does patient-ventilator asynchrony occur and what are the consequences?. , [J]. Respiratory Care 56(1), 25-38.
- 13.K G Mellott, M J Grap, C L Munro. (2014) Patient ventilator asynchrony in critically ill adults: frequency and types[J]. , Heart & Lung the Journal of Critical Care 43(3), 231.