
Abstract
Background and Aim
Gallbladder (GB) cancer is a highly fatal malignancy and approx. 10% new cases are diagnosed every year in India. The GB cancer has poor prognosis due to progressive nature. Understanding of risk factors that lead to GB development is urgently required for better management of the disease. Presence of stones in gall bladder generates varied mucosal reactions, which leads to different types of histopathological changes in mucosa. Here, our aim is to study the correlation between various types of mucosal responses e. g. inflammation, hyperplasia, metaplasia and carcinoma with different characteristics e. g. number and morphology of gallstones both in males and females.
Materials and Methods
A retrospective study of gallstones was performed on 438 cases of cholecystectomies operated laparoscopically based on the histological changes. Out of 438 cases, 394 (89.95%) were associated with gallstones and the rest 44 (10.05%) belonged to acalculous cholecystitis. The mucosal changes in calculous gall bladder were studied in 394 cases and its correlation with number and types of observed gallstones were evaluated. Tissue sections were taken from the fundus, body, neck and abnormal area of gallbladder for histopathological studies.
Results
Our study has revealed the higher incidence of inflammatory changes in males, while gall bladder hyperplasia, intestinal metaplasia and cancer cases were found mostly in females.
Conclusion
Our study showed that changes in the number and morphology of gallstones are directly associated with the mucosal changes in gallbladder e.g. inflammation, hyperplasia, metaplasia and gall bladder carcinoma.
Author Contributions
Academic Editor: Florin Graur, University of Medicine and Pharmacy "Iuliu Hatieganu" Cluj-Napoca, Romania.
Checked for plagiarism: Yes
Review by: Single-blind
Copyright © 2020 Vaishali V. Shirale, et al.
 This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Competing interests
The authors have declared that no competing interests exist.
Citation:
Introduction
Cholelithiasis induces diverse histopathological changes in the gallbladder mucosa e.g. acute & chronic inflammation, hyperplasia, granulomatous inflammation, cholesterosis, dysplasia, and carcinoma 1, 2. The overall incidence of Cholelithiasis in India is between 2% to 29% and mostly occurs in north than south India 3. Gall bladder mucosal changes depend upon the duration of cholelithiasis, size, number, stone type and gender of the patient 4. Coexistence of gallstones with cholecystitis, hyperplasia, intestinal metaplasia, and carcinoma is well known in literature 5. Incidental gallbladder (GB) carcinoma is revealed in 1% of all cholecystectomies done for benign conditions 6.Pathological stage of the disease decides the prognosis of the disease. Gall bladder metaplasia is characterized by intestinal or pyloric type epithelium found in association with cholelithiasis 7. Histopathological changes in the tissue can predict the chances of gall bladder cancer formation.
In a recent paper 8, it is found that as gallstone size increases, the response in gallbladder mucosa changes from cholecystitis, hyperplasia, and metaplasia to carcinoma. The Gallstone number and type are less important variables associated with these changes. In another study 9, the rate of incidental gallbladder carcinoma was found low in histopathological examination of cholecystectomies specimens. In India, the histopathological examination of Gallbladder specimens in Kumaon Region of Uttarakhand state has been completed 10.
Etiology and pathogenesis of GB cancer is not well known. The main difficulty in studying the precursor lesions of this disease is the fact that it is impossible to perform follow-up, because the diagnosis is established during surgery or after the cholecystectomy.
Therefore, the evidence relating these lesions to the cancer is determined indirectly. A better understanding of the risk factors for gall bladder cancer and premalignant lesions of the gall bladder could help in selection of prophylactic cholecystectomies and thus reduction in mortality 11. In the current study, we planned to correlate various gallstone characteristics (number and morphological type) with the type of mucosal response in gallbladder mucosa (inflammation, hyperplasia, metaplasia, and carcinoma).
Materials and Methods
No. of Patients & Tissue Collection
A retrospective study was conducted on 438 patients from a rural medical college between Jan 2018-Dec 2019, who underwent laparoscopic cholecystectomies. Out of 438 patients, 394 (89.95%) had gallstones and remaining 44 patients (10%) had acalculous cholecystitis. We examined the changes in the mucosa of calculous gall bladder for 394 patients (90%). Various parameters, (i) single or multiple (ii) type of morphology e.g. cholesterol/ pigmented/ combined/ mixed were used for evaluation of the gallstones. The histopathological examination was performed in four sections, (i) in two sections, tissue was taken from fundus and neck of the gall bladder and (ii) in other sections, tissue was taken from abnormal appearing mucosa. All sections were stained with hematoxylin and eosin.
Laparoscopic Surgery & Histopathological Examination
Abdominal ultrasound was performed to diagnose the cholecystolithiasis in all patients aged from 12-89 years old. In ultrasound, the gallbladder changes did not indicate the presence of GB cancer in any patient before preoperative stage. The surgeon conducted the macroscopic examination and laparoscopically removed the gallbladder. All tissues were subjected to histopathological analysis to examine the response e.g. inflammation, acute cholecystitis, chronic cholecystitis, empyema, xanthogranulomatous cholecystitis, hyperplasia, intestinal metaplasia, dysplasia, and malignant changes in gallbladder mucosa and its correlation with number and morphological type of stones.
Results
We examined the 438 cholecystectomy specimens, in which 394 cases (90%) belonged to gallstones and the rest 44 cases (10%) belonged to acalculous cholecystitis. We examined the mucosal changes in gallbladder for 394 cases to identify the correlation between mucosal changes and number and type of observed gallbladder stone. Out of 394 patients, 78 were males and 316 were females with M/F ratio 1:4. The observed mucosal changes in male and female patients are shown in Table 1. Figure 1, Figure 2, Figure 3.
Table 1. Observed mucosal changes in gallbladder of male and female patients| Type of lesion | Male | Female | Total | p-value |
| Chronic Cholecystitis | 57 | 284 | 341 | 0.004 |
| Acute cholecystitis | 4 | 1 | 5 | 0.004 |
| Cholesterosis | 3 | 6 | 9 | 0.004 |
| Follicular Cholecystitis | 0 | 0 | 0 | 0.004 |
| Xanthogranulomatous Cholecystitis | 7 | 9 | 16 | 0.004 |
| Papillary Hyperplasia | 1 | 3 | 4 | 0.004 |
| Adenomatoid Hyperplasia | 0 | 2 | 2 | 0.004 |
| Gastric Metaplasia | 0 | 2 | 2 | 0.004 |
| Intestinal Metaplasia | 6 | 8 | 14 | 0.004 |
| Carcinoma | 0 | 1 | 1 | 0.004 |
Figure 1.Photomicrographs showing A, Rokitansky agghste sinuses characteristic of chronic cholecystitis; B, Acute on Chronic Cholecystitis; C, Follicular Cholecystitis; D, Foamy macrophages admixed with mcaumulaig inflammatory infiltrate seen in Zbanikagmapincitma Cholecystitis (H&E)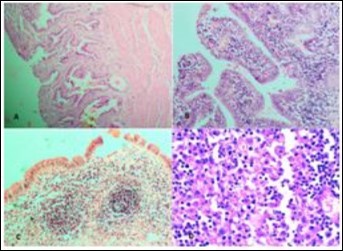
Figure 2.Photomicrograph showing A, cib;k%=Ss in low power; B, High power view of CiNk%=1%us showing lipid laden macrophages; C,ggtj of Gall Bladder; D, Pyloric Metaplasia Gall Bladder (H&E)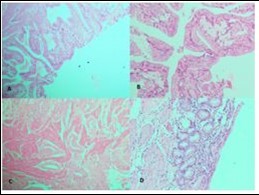
Figure 3.Photomicrograph showing A, Low power view of Adenocarcinoma Gall bladder; B, High power view shows attempted gland formation with moderate pleomorphismmoderately differentiated adenocarcinoma Gall Bladder; C, Low power view of Papillary carcinoma GB; D, High power view showing papillae with fibrovascular cores lined by malignant cells- Papillary carcinoma GB (H&E)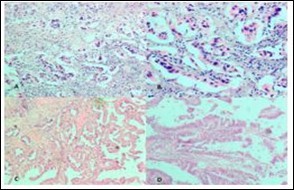
(Table 2) shows the type and number of stones observed in total 394 patients. Mixed type of stone was the most frequently encountered stone present in 276 cases (70.05%), which was predominantly multiple in numbers; followed by pigmented type around 77 cases (19.54%). Cholesterol stones were present in only 41 cases (10.40%). A total of 285 patients had multiple stones, while 109 patients had single stone.
Table 2. Correlation between morphological types and number of stones| No. Of Stones | |||
| Type of Stone | Single | Multiple | Total |
| Cholesterol | 23 | 18 | 41 |
| Mixed | 49 | 227 | 276 |
| Pigmented | 37 | 40 | 77 |
(Table 3) shows the various types of the mucosal changes observed in terms of number of stones. We studied the gall bladder mucosa microscopically and observed the most common change in chronic cholecystitis with cholelithiasis (341 cases, 86.54%). Xanthogranulomatous Cholecystitis was present in 16 cases (4%). Chronic Cholecystitis with metaplasia was present in 14 cases (3.55%), followed by Chronic Cholecystitis with focal cholesterosis in 9 cases (2.28%) Gall bladder carcinoma was found in 1 case (0.25%).
Table 3. Various types of mucosal changes in relation to number of stones| Number of Stones | p-value | |||
| Type of lesion | Single | Multiple | Total cases | |
| Chronic Cholecystitis | 92 | 249 | 341 | 2.6x10-12 |
| Acute cholecystitis | 0 | 5 | 5 | 2.6x10-12 |
| Cholesterosis | 4 | 5 | 9 | 2.6x10-12 |
| Follicular Cholecystitis | 0 | 0 | 0 | 2.6x10-12 |
| Xanthogranulomatous Cholecystitis | 5 | 11 | 16 | 2.6x10-12 |
| Papillary Hyperplasia | 2 | 2 | 4 | 2.6x10-12 |
| Adenomatoid Hyperplasia | 0 | 2 | 2 | 2.6x10-12 |
| Gastric Metaplasia | 1 | 1 | 2 | 2.6x10-12 |
| Intestinal Metaplasia | 5 | 9 | 14 | 2.6x10-12 |
| Carcinoma | 0 | 1 | 1 | 2.6x10-12 |
(Table 4) shows the correlation between mucosal changes and morphology of stones. We found that almost all the lesions were more common in gall bladders with multiple number of stones. It might be due to the fact that multiple stones are far more common than single (63.47%) and irritation of mucosa is greater with higher number of stones. Among the other changes, multiple stones were more associated with cholecystitis, xanthogranulomatous cholecystitis, in both gastric and intestinal metaplasia, as shown in Table 4.
Table 4. Correlation of mucosal changes with morphology of stones| Type of Stone | ||||
| Type of lesion | Cholesterol | Mixed | Pigmented | Total |
| Chronic Cholecystitis | 39 | 249 | 53 | 341 |
| Acute cholecystitis | 1 | 2 | 2 | 5 |
| Cholesterosis | 1 | 2 | 6 | 9 |
| Follicular Cholecystitis | 0 | 0 | 0 | 0 |
| Xanthogranulomatous Cholecystitis | 0 | 9 | 7 | 16 |
| Papillary Hyperplasia | 0 | 1 | 3 | 4 |
| Adenomatoid Hyperplasia | 0 | 2 | 0 | 2 |
| Gastric Metaplasia | 0 | 1 | 1 | 2 |
| Intestinal Metaplasia | 0 | 9 | 5 | 14 |
| Carcinoma | 0 | 1 | 0 | 1 |
In the current work, a retrospective study on 394 patients was carried out to find the correlation between gallstones (number and morphology) with mucosal changes that occur in the gall bladder. It is already known that cholecystolithiasis is associated with GB cancer, as cholecystolithiasis is observed in 80% of all GB cancer cases 12. In one study, incidence of GB cancer is about 1.68%, whereas it is 3.5% in another study in which multiple histopathological sections of GB was examined 13. Coexistence of cholecystolithiasis with xantho granuloma to us cholecystitis, adenomyomatosis, pyloric and intestinal metaplasia is well known in literature 14. In our study, majority of patients were aged between 30 to 39 years. The females are more sufferers than males, as 1:4 (Male/Female) GB stone incidence is observed in various studies 15, 16.
Mixed stones incidence (70.05%) was most commonly observed gallstone in North India and also observed in our study 15, 17. We observed 19.54% (77/394) pigmented stones, 10.40% (41/394) cholesterol stones, 72.33% (285/394) multiple mixed stones and 27.66% (109/394) single stones, as observed in other reports 11, 18, 19. These data indicate that cases with multiple stones are more symptomatic (cholecystitis) than single stone and mucosal changes e.g. hyperplasia, metaplasia, and carcinoma are more common with multiple mixed stones. Dysplasia and carcinoma in situ were detected in 16/394 (4%) and 1/394 (0.25%) patients, when we examined the multiple sections of gall bladder from fundus, body, and neck.
Precancerous gall bladder mucosal changes are important clinically as well as pathologically, however not studied carefully by pathologist earlier 20. We observed gall bladder mucosal hyperplasia in 6/394 (1.5%) cases in females only. The primary cholelithiasis causes mechanical mucosal irritation and results in hyperplasia. Intestinal metaplasia was detected in only 14/394 cases (3.5%).
Higher incidence of cholecystolithiasis was observed in females compared to males, which causes increased risk of gall bladder cancer. This may be due to decrease in activity of cholesterol reductase and increase in activity of HMG-CoA reductase with age, resulting in increased cholesterol secretion and saturation of bile. The female sex hormones may also expose them to factors that possibly promote the formation of gallstones. Early menarche, early first pregnancy, multiple pregnancies, and delayed menopause may increase the risk of gall bladder carcinoma 12.
An earlier study 25 suggested that gallbladder metaplasia changes are found commonly in patients with multiple mixed stones. This association seems to be relative and statistical association could not be demonstrated between number of stones and mucosal response 26. Xanthogranulomatous cholecystitis is an uncommon inflammatory and destructive gall bladder process that can spread to adjacent structures and could be confused with cancer. This histological alteration occurs in approximately 2.9% of all cholecystectomies, affects men and women equally and is frequently associated with gallstones. The occurrence of cancer in gall bladders with xanthogranulomatous cholecystitis has been reported and has been observed in 9-12% of these cases. Similarly, xanthogranulomatous cholecystitis presented a higher incidence within elderly individuals in this study and, interestingly, occurred more often among women.
In our study, the incidence of acute cholecystitis was higher in males as observed in other study 27. The incidence of cholecystolithiasis and GB cancer increases with age. An estimated 0.25% of the patients above 65 with cholecystolithiasis may develop GB carcinoma, that depends upon the duration of gallstone disease than the age of patient 28. We observed 1/394 case of GB carcinoma.
Adenomatoid hyperplasia, a non-inflammatory benign gall bladder alteration, mostly occurred in middle aged patients and increased with age. It is presently identified as a precancerous lesion, and cancer cases associated with adenomyomatosis have been reported in literature 29.
In our study, we observed that metaplasia and dysplasia increased with age and the metaplastic alterations and dysplasia are taken as precancerous lesions. The gall bladder cancer is an extremely slow progressive disease and prolonged follow up may be needed 18. Ransohoff and Gracie 30 performed the follow-up of 123 patients with asymptomatic cholecystolithiasis for seven years without any symptoms of GB cancer. Maringhini and associates performed follow-up on 2,583 patients for 13 years, however five patients (0.2%) developed cancer in this period.
Whether prophylactic cholecystectomy should be performed in asymptomatic gallstones is a matter of debate. However, an Indian study recommends prophylactic cholecystectomies for asymptomatic gallstones in young patients with thickened GB wall (greater than 3 mm), with large gallstones (greater than 3 cm), patients with porcelain GB, sessile polyps (greater than 1 cm) and in people from areas with high incidence rates of GB cancer 31.
Our study advocates that there is correlation between gall bladder stones and gall bladder histological changes. Nonetheless, further work is needed to understand about various risk factors of gall bladder cancer. Our data is crucial to establish the surgical treatment for various pathological gall bladder conditions e.g. symptomatic or asymptomatic calculous cholecystitis.
Conclusion
Our study showed that patients with multiple gallstones were more symptomatic (cholecystitis) than with single stone. The mucosal changes like hyperplasia, metaplasia, and carcinoma were also more common in cases with multiple mixed type of stones. Etiology or pathogenesis of multiple stones were more symptomatic (cholecystitis) than with single stone and mucosal changes like hyperplasia, metaplasia, and carcinoma were also more common in cases with multiple mixed type of stone. Still, we require further studies to understand gall bladder stones leading to carcinogenesis and risk factors.
References
- 2.Baidya R, Sigdel B, Baidya N L. (2012) Histopathological changes in gallbladder mucosa associated with cholelithiasis. , J Pathol Nepal 2, 224-5.
- 3.Mohan H, Punia R P, Dhawan S B, Sekhon M S. (2005) Morphological spectrum of gallstone disease in 1100 cholecystectomies in North India. , Indian J Surg 67, 140-2.
- 4.GoyalS Singla, DuhanA. (2014) Correlation between gallstones characteristics and gallbladder mucosal changes: A retrospective study of 313 patients. , Clin Cancer Investig J 157-161.
- 5.Xeropotamos N, Skopelitou A S, Batsis C H, Kappas A M. (2001) Heterotopic gastric mucosa together with intestinal metaplasia and moderate dysplasia in the gall bladder: report of two clinically unusual cases with literature review. Gut. 48, 719-727.
- 6.Shrestha R, Tiwari M, Ranabhat S K, Aryal G. (2010) Rauniyar SK and Shrestha HG Incidental gallbladder carcinoma: value of routine histological examination of cholecystectomy specimens. , Nepal Med Coll J 12(2), 90-94.
- 7.Albores-Saavedra J, Nadji M, Henson D E, Ziegels-Weissman J, Mones J M. (1986) Intestinal metaplasia of the gallbladder: A morphologic and immunocytochemical study. Hum Pathol. 17, 614-620.
- 8.Singh A, Singh G, Kaur K, Goyal G, Saini G et al. (2019) Histopathological Changes in Gallbladder Mucosa Associated with Cholelithiasis: A Prospective Study. , Niger J Surg 25(1), 21-25.
- 9.Charfi S, Gouiaa N, Mnif H. (2018) Histopathological findings in cholecystectomies specimens: A single institution study of 20 584 cases. , HepatobiliaryPancreatDis Int 17(4), 345-348.
- 10.Shukla S K, Pant P, Singh G, Shahi KS Bhuvan. (2020) . Histopathological Examination of Gallbladder Specimens in Kumaon Region of Uttarakhand. JGastrointestCancer 51(1), 121-129.
- 11.Costa A L, Bresciani C J, Perez R O, Bresciani B H, Sigueria S A et al. (2010) Are histological alterations observed in the gallbladder precancerous lesions? Clinics (Sao Paulo). 65, 143-150.
- 12.Costa A L, Bresciani C J, Perez R O, Bresciani B H, Sigueria S A et al. (2010) Are histological alterations observed in the gallbladder precancerous lesions? Clinics (Sao Paulo). 65, 143-150.
- 13.Jukemura J, Leite K R, Machado M C, Montagnini A L, Penteado S et al. (1997) Frequency of incidental gallbladder carcinoma in Brazil. ABCD Arq Bras Cir Dig. 12, 10-13.
- 14.Loyd R A, Rujirakul R, Panpimanmas S. (2016) Helicobacter Species is Possible Risk Factors of Cholangiocarcinoma. , Asian Pac J Cancer Prev 17(1), 37-44.
- 15.Mohan H, Punia R P, Dhawan S B, Sekhon M S. (2005) Morphological spectrum of gallstone disease in 1100 cholecystectomies in north India. , Indian J Surg 67, 140-142.
- 16.Khanna R, Chansuria R, Kumar M, Shukla H S. (2006) Histological changes in gallbladder due to stone disease. , Indian J Surg 68, 201-204.
- 17.Tyagi S P, Tyagi N, Maheshwari V, Ashraf S M, Sahoo P. (1992) Morphological changes in diseased gall bladder: A study of 415 cholecystectomies at Aligarh. , J Indian Med Assoc 90, 178-181.
- 18.Domeyer P J, Sergentanis T N, Zagouri F, Tzilalts B, Mouzakioti E et al. (2008) Chronic cholecystitis in elderly patients. Correlation of the severity of inflammation with the number and size of the stones. In Vivo. 22, 269-272.
- 19.Juvonen T, Niemela O, Makela J, Kairaluoma M I. (1994) Characteristics of symptomatic gall bladder disease in patients with either solitary or multiple cholesterol gallstones. Hepatogastroenterology. 41, 263-266.
- 20.Mukuda T, Andoh N, Matsushiro T. (1985) Precancerous lesions of the gallbladder mucosa. , Tohoku J Exp Med 145, 387-94.
- 21.Yamagiwa H, Tomiyama H. (1986) Intestinal metaplasia-dysplasia-carcinoma sequence of the gallbladder. , Acta Pathol Jpn 36, 89-97.
- 22.rd. (1987) Gallstones, gallbladder cancer and other gastrointestinal malignancies. An epidemiologic study in Rochester. , Minnesota, Ann Intern Med 107, 30-35.
- 23.Tazuma S, Kajiyama G. (2001) Carcinogenesis of malignant lesions of the gallbladder. The impact of chronic inflammation and gallstones. Lagenbecks Arch Surg. 386, 224-229.
- 24.Kayahara M, Nagakawa T. (2007) Recent trends of gallbladder cancer in Japan: An analisis of 4770 patients. , Cancer 110, 572-580.
- 25.Lee1 H K, Han H S, Min S K, Lee J H. (2005) Sex-based analysis of the outcome of laparoscopic cholecystectomy for acute cholecystitis. , British Journal of Surgery 92, 463-466.
- 26.Roa I, X de Aretxabala, Araya J C, Roa J. (2006) Preneoplastic lesions in gallbladder cancer. , J Surg Oncol 93, 615-623.
- 27.Lam C M, Yuen A W, Wai A C, Leung R M, Lee A Y et al. (2005) Fan Gallbladder ST. Cancer presenting with acute cholecystitis a population-based study. Surg Endosc. 19, 697-701.
- 28.Sheth S, Bedford A, Chopra S. (2000) Primary gallbladder cancer: Recognition of risk factors and the role of prophylactic cholecystectomy. , Am J Gastroenterol 95, 1402-1410.
- 29.Aldridge M C, Gruffaz F, Castaing D, Bismuth H. (1991) Adenomyomatosis of the gallbladder. A premalignant lesion?. , Surgery 109, 107-110.