
Abstract
Background:
Medullary Thyroid Cancer (MTC) is a rare malignancy, accounting for less than 3% of all thyroid cancers and causes significant morbidity and mortality. MTC is often due to an underlying mutation of the RET proto-oncogene, which can result in additional endocrinopathies that must be screened for pre-operatively. The project aim was to determine if surgical training background influenced patient pre-operative evaluation for MTC.
Methods:
A retrospective review was performed of patients undergoing thyroidectomy for MTC at a single academic institution. Patients were analyzed based on who performed the initial operative procedure, a surgeon with specific endocrine surgery training or a surgeon without.
Results:
From 1994 to 2011, 37 patients with MTC were identified. Thirty percent were managed by an endocrine surgeon and 70% by a non-endocrine surgeon. A complete thyroid work-up was done for all the patients managed by an endocrine surgeon vs. 38.5% of the non-endocrine surgeon patients (p<0.01). Appropriate preoperative endocrine screening was performed in 91% of the endocrine surgeon patients vs. 50% of the non-endocrine surgeon patients (p= 0.03). RET mutation genetic testing was done for all endocrine surgeon patients vs. 85% of non-endocrine surgeon patients (p= 0.30).
Conclusion:
Endocrine trained surgeons recognize and appropriately manage the complexity of MTC and associated endocrinopathies, more often than surgeons without an endocrine surgery background. This may result in optimized management of these patients.
Author Contributions
Academic Editor: Giovanni Mauri, IRCCS Policlinico San Donato Unit of Radiology; Milan, Italy
Checked for plagiarism: Yes
Review by: Single-blind
Copyright © 2015 Amal Alhefdhi, et al.
 This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Competing interests
The authors have declared that no competing interests exist.
Citation:
Introduction
The number of thyroid and parathyroid procedures being performed in the United States has been steadily increasing over the last few years, with 80,505 cases being done in 2004, an increase of over 16,000 operations in 4 years 1. It is estimated that a minimum of 97,700 cases will be performed in 2020, but it may be as high as 173,509 procedures 1, 2. With the growing number of thyroid and parathyroid procedures, there is an increasing need to train surgeons in the field of endocrine surgery 3. Therefore, endocrine surgery is recognized as an important subspecialty of general surgery 4.
Bilimoria et al looked at thyroidectomies performed for thyroid cancer using the National Cancer Center Database and showed that only 8% of thyroid cancer patients were treated at a designated National Comprehensive Care Network/National Cancer Institute center, with another 41% at other academic hospitals and 59% at community hospitals 5. However, the management of patients with surgical endocrine disease is intellectually stimulating and often complex, requiring a multidisciplinary team of endocrinologists, radiologists, pathologists, and surgeons 6, 7.
Medullary thyroid carcinoma (MTC) is a neuroendocrine (NE) tumor that originates from the calcitonin-secreting para-follicular C cells found within the thyroid. MTC is a relatively rare malignancy, accounting for less than 3% of all thyroid cancers. As it is locally aggressive and metastasizes early, it is associated with significant morbidity and mortality 8. One fourth of all MTC appears to be genetically determined and is associated with an inherited clinical syndrome (multiple endocrine neoplasia 2A, and 2B and familial MTC). The remaining cases of MTC are sporadic and therefore occur as the consequence of somatic alterations caused by both genetic and epigenetic factors 9.
The aim of the present study was to determine if surgeon training and knowledge of the unique aspects of this rare disease may influence the adequacy of the preoperative evaluation. We hypothesize that surgeons who have been specifically trained in endocrine surgery will be more apt to look for associated endocrinopathies and optimize the surgical management of patients with this rare disorder.
Methods
A review of a prospective surgical database from to was performed on all patients undergoing thyroidectomy or neck dissection at an academic tertiary referral center. Patients with a pathologic or cytologic diagnosis of MTC or who tested positive for RET (rearranged during transfection) mutations were identified. Patients were subdivided into two groups based on the specialty of the surgeon who did their initial operation: those with an initial surgery by an endocrine trained surgeon and those with an initial surgery by a non-endocrine trained surgeon (general surgeon or otolaryngologist without dedicated endocrine training). All the surgeons performed thyroidectomy as a regular part of their practice.
The institutional electronic medical record was reviewed to determine the extent of preoperative thyroid evaluation (ultrasound, fine needle aspiration, and serum calcitonin level), endocrine workup (to rule out possible associated endocrinopathies) and genetic testing for the RET mutation. Patients generally presented in one of two ways, and for this reason, the extent of thyroid work up needed varied. An appropriate thyroid work up for patients presenting with either a known RET mutation, positive family history or personal history of pheochromocytoma or primary hyperparathyroidism suggestive of MEN2, consisted of baseline thyroid function, as well as a serum calcitonin level. Patients with calcitonin levels less than 2 pg/mL were not required to undergo thyroid ultrasound. An appropriate work up for those patients presenting with a thyroid nodule consisted of baseline thyroid function, thyroid ultrasound with fine needle aspiration (FNA) where indicated. Once the diagnosis of MTC was made or suspected based on the FNA results, further work up including serum calcitonin, and CEA levels was performed.
Once the diagnosis of MTC was suspected or confirmed in the pre-operative period, a specific work up in regards to associated endocrinopathies required checking metanephrines (either plasma or urinary) to rule out synchronous pheochromocytoma, and serum calcium level to rule out synchronous primary hyperparathyroidism. Appropriate genetic testing consisted of screening for a mutation in the RET proto-oncogene, or testing for the known familial mutation for those individuals with a positive family history. Patients were considered to be in a high risk group for MTC, if the patient had any the following criteria: positive family history or personal history of pheochromocytoma or primary hyperparathyroidism suggestive of MEN2, or if the patient is known to have a RET mutation, or if the calcitonin level was elevated.
Statistical analysis was performed using Fisher’s exact test and unpaired t-test, as appropriate. Calculations were completed using SPSS version 17 (SPSS Inc, Chicago II). A p-value of ≤ 0.05 was considered significant.
Results
Between 1994 and 2011, thirty-seven patients underwent thyroidectomy for MTC. Females accounted for 54% (n= 20) of the total patients. The mean age was 25 ± 22 years. Eleven (30%) patients were managed by surgeons with formal endocrine surgery training, while the remaining majority (n=26, 70%) was managed by surgeons without formal endocrine surgery training. There were no differences between the two groups in form of gender and age (Table 1). Patients treated by an endocrine surgeon were more likely to have appropriate
preoperative thyroid workup 11 (100%) vs. 10 (38.5%) (p= < 0.001, Table 1, and Figure 1). All of the 16 patients without a complete preoperative thyroid work up were missing thyroid ultrasound in spite of at least one high risk patient criteria being present. Preoperative calcitonin was performed in 10 (91%) of the endocrine surgeon patients versus 14 (54%) of the non-endocrine surgeon patients (p=0.06, Table 1, and Figure 2). Among the 12 patients who did not have a preoperative calcitonin level measured, 11 had at least one positive high risk criteria (Figure 2).
Table 1. Patients Data| Endocrine trained surgeon | Non-endocrine trained surgeon | P value | |
| Demographic data | |||
| Total number of cases | 11 (30%) | 26 (70%) | <0.01 |
| Female/Male | 5/6 (46%) | 15/11 (59%) | 0.72 |
| Age* (Year) | 2 ± 11 | 17 ± 18 | 0.61 |
| Patients workup summary | |||
| Complete Thyroid work-up | 11 (100%) | 10 (39%) | 0.01 |
| Preoperative Calcitonin | 10 (91%) | 14 (54%) | 0.06 |
| Complete Endocrine work-up | 10 (91%) | 13 (50%) | 0.03 |
| Pre/postoperative Genetic test | 11 (100%) | 23 (89%) | 0.54 |
Figure 1.Preoperative Thyroid Work up. *No ultrasound (US) in present of positive family history or personal history of pheochromocytoma or primary hyperparathyroidism suggestive of MEN2, or the patient is known to RET mutation, or calcitonin level was high.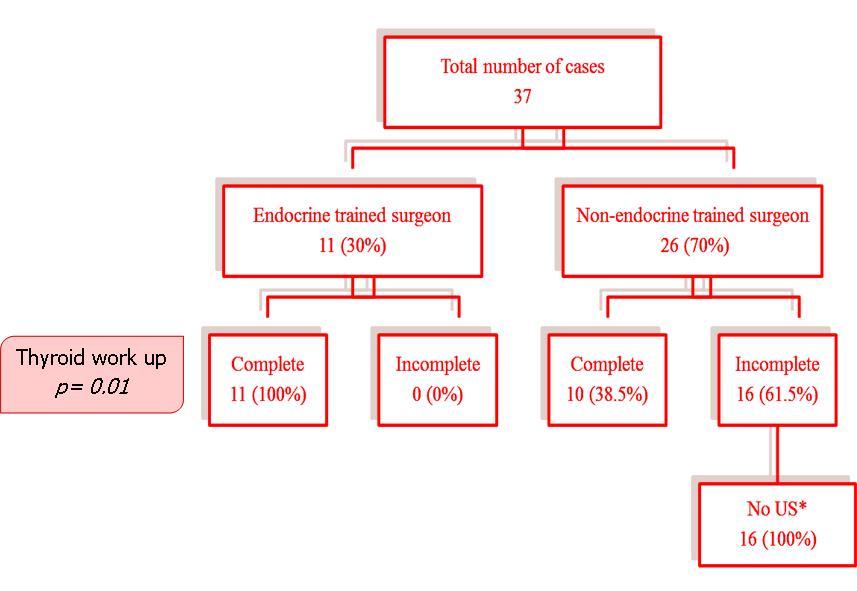
Figure 2.Preoperative Calcitonin Data. * Criteria in favor of MTC include positive family history or personal history of pheochromocytoma or primary hyperparathyroidism suggestive of MEN2, or the patient is known to RET mutation, or calcitonin level was high.
An appropriate preoperative endocrine workup, consisting of the measurement of metanephrines (urine or plasma) and serum calcium, was done for 10 (91%) of the endocrine surgeon patients, and only 13 (50%) of the non-endocrine surgeon patients (p= 0.03, Table 1). Among the 13 patients who did not have a complete preoperative endocrine work up, 11 patients had at least one high risk criteria (Figure 3). Genetic testing for a RET mutation was performed for all endocrine surgeon patients, while only 23 (89%) of the non-endocrine surgeon patients underwent genetic testing (p= 0.54, Table 1, Figure 4). Of the three patients who did not have genetic testing performed, all had positive FNAs for MTC, with confirmatory MTC in the final pathology. One was offered genetic testing by endocrinology in follow up but the patient refused the other two never had genetic testing performed or offered.
Figure 3.Preoperative Endocrine Work up Data. * Criteria in favor of MTC include positive family history or personal history of pheochromocytoma or primary hyperparathyroidism suggestive of MEN2, or the patient is known to RET mutation, or calcitonin level was high.
Figure 4.Genetic Testing Data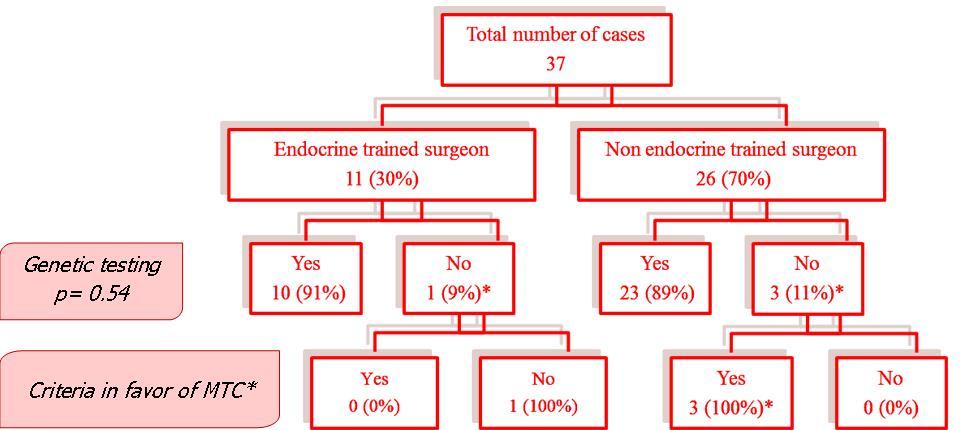
Discussion
Medullary thyroid cancer is a rare malignancy and is unique in that it is associated with a genetic mutation in approximately 20% of cases which can be associated with other endocrinopathies, which can be life-threatening if not recognized and dealt with appropriately prior to treatment of their primary thyroid tumor 10, 11. Therefore, we hypothesized that surgeons with training not only in the technical aspects of thyroidectomy, but in endocrine surgery, would have a better understanding of the unique aspects of this disease and hence would provide more comprehensive initial care. We found that patients operated on by an endocrine trained surgeon were much more likely to get an appropriate thyroid and endocrine workup preoperatively and to refer their patients for genetic testing.
The findings of this study are the first regarding the potential impact of endocrine surgery training in the pre-operative evaluation of MTC, and echo previous studies highlighting the value of endocrine surgical subspecialty training 1, 12, 13, 14. This study showed that preoperative thyroid work up, and screening for endocrinopathies was significantly more likely to be performed when the initial surgery was done by an endocrine trained surgeon versus a non-endocrine trained surgeon. Thus, this study demonstrates that endocrine trained surgeons recognize and appropriately manage the complexity of MTC, and associated endocrinopathies, more often than surgeons without an endocrine surgery background. This may result in optimized management of these patients.
The result of this study is in agreement with previous studies that demonstrate the relationship between surgical outcomes and surgical specialty training. For example, mortality is lower for both gastrectomies and colectomies when performed by subspecialty trained surgeons, even after accounting for hospital and surgeon volume and patient characteristics 15. Moreover, specialty training in thoracic surgery has an independent association with lower mortality after esophageal resection. Although in their study specialty training was less important than hospital and surgeon volume 16. Such results may have implications for surgical subspecialty training programs and for regionalization of complex surgical procedures 17.
The complexity of surgical science and surgical patient care is growing rapidly. As a result of that, many areas which were under the scope of general surgery practice have developed into separate specialties with unique advanced training requirements 18. Core training for surgeons in any surgical specialty should include: education in the relevant basic science knowledge, training in fundamental diagnostic skills, development of surgical technical skills and considerable experience in patient care 19. In order to effectively treat a patient with MTC, it is important for a surgeon to not only understand the clinical disease, but the genetics behind it and the molecular pathways that are affected. RET proto-oncogene germline mutations have been found in almost all hereditary cases of MTC, while somatic RET mutations are found in up to 50% of sporadic MTCs 11, 20, 21. Moreover, there is a genotypic/phenotypic correlation between the type of RET mutation and the clinical features 11, 20, 21. Growth factors, such as the epidermal growth factor receptor (EGFR), the vascular endothelial growth factor receptor (VEGFR) and VEGFR-2 have been found to be overexpressed in MTC, and to play a role in cancer development, metastasis and progression 20. In addition, the fibroblast growth factor receptor 4 (FGFR4) has been reported to be overexpressed in MTC cell lines, and the platelet-derived growth factor receptor (PDGFR) seems to play a role in differentiated thyroid cancer, but its role have not been fully investigated in MTC 20.
Further sub-specialization is likely inevitable, if the discipline of General Surgery is to remain a desired specialty. Endocrine surgery has evolved into a sub-specialty of General Surgery, and over the last few decades has matured as a discipline. With this maturation comes the responsibility of defining the gold standard of care to be provided by surgeons involved in the care of patients with endocrine diseases 22.
Historically, a high percentage of endocrine surgical procedures are performed by general surgeons or otolaryngologic surgeons in nonteaching environments 23. Sophisticated work-force projections suggest that the supply of endocrine surgeons will grow over the next 15 years, but will be outpaced by the anticipated demand. Therefore it is likely that a significant amount of thyroid surgery will continue to be done by non-endocrine trained surgeons 24. Therefore it is important for us to know which patients can benefit the most from referral to a dedicated endocrine surgeon.
There are several limitations to our study. Due to the rarity of MTC, our study population is relatively small and also represents only a single institution’s experience. The other challenge is that a pre-operative diagnosis of MTC is not always apparent; therefore it is not always feasible to obtain an endocrine work up preoperatively. However, in our review of the cases without an endocrine workup preoperatively, the preoperative diagnosis suggested MTC in the majority of the cases. Therefore it is essential that clinicians have a high index of suspicion so that the appropriate work up can be done whenever feasible. Insurance coverage of RET testing can be variable, but in the cases in which genetic testing was not obtained, we could find no documentation that insurance coverage was a limiting factor.
Conclusion
Surgeons need to recognize the risk of associated endocrinopathies in order to optimize outcomes for patients with MTC. Endocrine surgeons, who are trained not only in thyroid surgery, but to deal with complexity of this disease, play an important role in optimizing treatment for patients with MTC. Surgeons with specific endocrine surgery training are more likely to complete the complex preoperative work up for patients with MTC.
Acknowledgements
Ministry of higher education of Saudi Arabia, and King Faisal Hospital & Research Center (KFSH&RC), Riyadh, Saudi Arabia, scholarship.
References
- 1.Sosa J, Wang T, Yeo H. (2007) The maturation of a specialty: Workforce projections for endocrine surgery. Surgery. 142(6), 876-83.
- 2.Saunders B, Wainess R, Dimick J. (2003) Who performs endocrine operations in the United States? Surgery. 134(6), 924-31.
- 3.Harness J, Organ C J, Thompson N. (1995) Operative experience of U.S. general surgery residents in thyroid and parathyroid disease. Surgery. 118(6), 1063-9.
- 4.Goldfarb M, Gondek S, Hodin R. (2010) Resident/fellow assistance in the operating room for endocrine surgery in the era of fellowships. SURGERY. 148(6), 1065-1072.
- 5.Bilimoria K Y, Bentrem D J, Linn J G. (2007) Utilization of thyroid surgery for papillary thyroid cancer in the United States. Surgery;142: 906-13.
- 7.Sosa J, Bowman H, Tielsch J. (1998) The importance of surgeon experience for clinical and economic outcomes from thyroidectomy. , Ann 228(3), 320-30.
- 8.Ningle L, Greenblatt D, Kunnimalaiyaan M. (2008) Suberoyl Bis-Hydroxamic Acid Activates Notch-1 Signaling and Induces Apoptosis in Medullary Thyroid Carcinoma Cells. The Oncologist. 13, 98-104.
- 9.Dilla T, Velasco J, Medina D. (2000) The MDM2 Oncoprotein Promotes Apoptosis in p53-Deficient Human Medullary Thyroid Carcinoma Cells. , Endocrinology; 141, 420-429.
- 10.Zhou P, Liu J, Cheng S W.(Jun2012) Hereditary medullary thyroid carcinoma: the management dilemma. , Fam Cancer; 11(2), 157-65.
- 11.Antonelli A, Fallahi P, Ferrari S M.( Apr2012) RET TKI: potential role in thyroid cancers. , Curr Oncol 14(2), 97-104.
- 12.Solorzano C C, J A Sosa, S C Lechner.Endocrine surgery: Where are we today? A national survey of young endocrine surgeons. , Surgery; 147(4), 536-541.
- 13.Karmali S, Harness J K, Sheppard B C, D Le.(Feb2008) An Update: The Operative Experience in Adrenal, Pancreatic. , and Other Less Common Endocrine Diseases of U.S. General Surgery Residents. World J Surg; 32(2), 232-6.
- 14.Harness J K, van Heerden JA, Lennquist S.Future of thyroid surgery and training surgeons to meet the expectations of 2000 and beyond.WorldJSurg;. 24(8), 976-82.
- 15.Y J Jang, M S Park, Park S S. (2010) Surgeon Subspecialty as a Factor in Improving Long-term Outcomes for Gastric CancerTwenty Years of Experience in Korea. Arch Surg. 145(11), 1091-1096.
- 16.J B Dimick, Goodney P P, Orringer M.Specialty Training and Mortality After Esophageal Cancer Resection. Ann Thorac Surg 2005;80:. 282-6.
- 17.M A Callahan, P J Christos, H T Gold.(Oct2003) Influence of Surgical Subspecialty Training on In-Hospital Mortality for Gastrectomy and Colectomy Patients. Ann Surg;. 238(4), 629-639.
- 18.Bass B L.(Dec2006) Early specialization in surgical training: an old concept whose time has come? Semin Vasc Surg;. 19(4), 214-217.
- 19.Potts J R.(Dec2006) 3rd. Core training in surgery: what does it need to include? Semin Vasc Surg;. 19(4), 210-213.
- 20.Giunti S, Antonelli A, Amorosi A. (2013) Cellular signaling pathway alterations and potential targeted therapies for medullary thyroid carcinoma. , Int J Endocrinol; 2013, 803171.
- 21.Fallahi P, Ferrari S M, Santini F.(Dec2013) Sorafenib and thyroid cancer. , BioDrugs; 27(6), 615-28.
- 22.Pasieka J L.(Mar2005,1) Kindred spirits of the endocrines: The training of the future endocrine surgeons. , J. Surg. Oncol; 89, 202-205.